

Volume 12, Issue 3 (September 2025)
Avicenna J Neuro Psycho Physiology 2025, 12(3): 166-171 |
Back to browse issues page

Ethics code: IR.RAZI.REC.1404.016
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rafiee S, Momeni K, Yazdanbakhsh K, Foroughi A. Psychometric Properties of Persian Version of Negative Self-Compassion Beliefs Scale: A Study among Overweight and Obese Individuals. Avicenna J Neuro Psycho Physiology 2025; 12 (3) :166-171
URL: http://ajnpp.umsha.ac.ir/article-1-541-en.html
URL: http://ajnpp.umsha.ac.ir/article-1-541-en.html



1- Department of Psychology, Razi University, Kermanshah, Iran.
2- Faculty of Social Sciences, Department of Psychology, Razi University, Kermanshah, Iran. ,kh.momeni@razi.ac.ir
3- Faculty of Social Sciences, Department of Psychology, Razi University, Kermanshah, Iran.
4- Department of Clinical Psychology, School of Medicine, Kermanshah University of Medical Sciences, Kermanshah, Iran.
2- Faculty of Social Sciences, Department of Psychology, Razi University, Kermanshah, Iran. ,
3- Faculty of Social Sciences, Department of Psychology, Razi University, Kermanshah, Iran.
4- Department of Clinical Psychology, School of Medicine, Kermanshah University of Medical Sciences, Kermanshah, Iran.
Full-Text [PDF 431 kb]
(122 Downloads)
| Abstract (HTML) (743 Views)
Table 1. Means and Standard Deviations of participants by Gender
Table 2. Fit indices of the one factor model of the NSCB-S
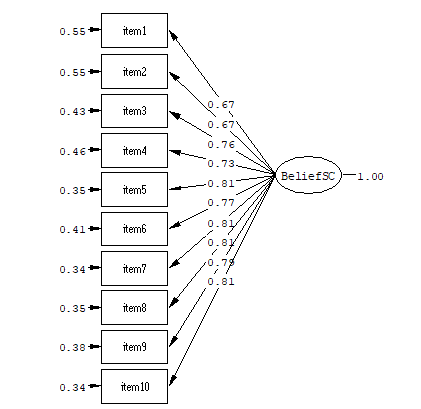
Table 3. Convergent and Divergent Validity of Negative Self-Compassion Beliefs scale
Full-Text: (121 Views)
Background
Weight management is emotionally challenging. Results show that approximately 42% of adults in the general population attempt to lose weight, while about 23% report attempting to maintain their weight [1, 2]. Most obese people experience higher distress and self-blame regarding their excess weight, particularly if they have encountered previous failures in weight-loss attempts or have been unable to achieve their desired body shape [3, 4]. On the other hand, overweight and obesity often function as social markers, perceived as indicators of personal failure to control weight [5], lack of willpower and self-indulgence, sloth, and gluttony [6]. They are also associated with depressive and anxiety symptoms, dysfunctional attitudes and behaviours, and internalized weight bias [5].
Self-compassion is an emerging component of weight management intervention. This approach is designed to cultivate a kind and accepting relationship with oneself during distress or emotional challenges [2], such as distress related to obesity [7]. Self- compassion is positively associated with self-efficacy, and promotes more adaptive emotional responses to dietary relapses [8, 9]. It can have a salient and beneficial effect on weight- and body image-related problems, and eating disorder behaviours in both clinical and non-clinical samples [10-13].
Empirical evidence suggests that self-compassion-based abilities may serve a protective role against body dissatisfaction, body shame, body monitoring, and severity of disordered eating [14-16]. Self-compassionate individuals tend to adaptively cope with a range of emotionally challenging situations, including those for which they are not at fault [17, 18].
Furthermore, self-compassion is linked to greater intentions for self-improvement following difficulties [18, 19], improved coping with insurmountable obstacles, reduced negative attitudes toward overeating after an unsuccessful attempt [20], lower weight stigma [21], and decreased binge eating [22].
Despite its benefits, many individuals encounter barriers to self-compassion and find its techniques difficult to implement [23]. These barriers include fear of self-compassion and refrain from practicing it [24], negative physiological responses to self-compassion exercises [15, 25], perception of self-compassion as a weakness, painful memories associated with lack of compassion in the past, feeling of unworthiness [26], and being overwhelmed by sadness when experiencing self- kindness [27].
A further major obstacle is the presence of “negative self-compassion beliefs”— the beliefs that self-compassion leads to less motivation, increased self-indulgence, and diminished self-responsibility. These beliefs are considered a primary barrier to engaging in self-compassion practices [28-30]. Such beliefs can become self-fulfilling, as individuals who endorse them may avoid self-compassion in emotionally challenging situations. Conversely, individuals who do not hold these negative beliefs or who have been primed in a way that reduces such beliefs, may be more inclined to practice self-compassion in difficult times and challenging situations, which is related to more adaptive coping and greater self-improvement intentions [31].
Objectives
Objectives
According to Gilbert (2011) and Neff and Germer (2013) works, Chwyl et al. (2020) operationalized three key negative self-compassion beliefs: the belief that self-compassion leads to complacency, self-indulgence, and decreased self-responsibility [31]. This scale comprises 10 items that are measured on a Likert scale, from strongly disagree to strongly agree. Their study supported a single factor structure [31]. Considering their study [31] and a recent systematic review [32], although self-compassion-based interventions have been effective in weight management, maintaining these gains in the long term remains unclear and has several barriers (e.g., negative beliefs and fears about self-compassion). However, to the best of the researchers’ knowledge, no study has yet specifically examined negative self-compassion beliefs among overweight individuals. Consequently, the present study aimed to answer the following question: Does the Negative Self-Compassion Beliefs Scale (NSCB-S) have adequate divergent and convergent validity among overweight individuals?
Materials and Methods
This quantitative study was performed with 207 overweight individuals who had referred to Kermanshah Nutrition Clinics between June and September 2025 (149 women, 72%, and 58 men, 28%). Following Klein’s (2010) recommendation for structural equation modelling, a sample size of at least 200 people is defensible [33]. Participants (n=207) were selected through convenience sampling from nutrition clinics. The sample consisted of overweight and obese individuals. Inclusion criteria were fluency in Persian and a body mass index (BMI) over 25 kg/m2. Exclusion criteria included “Unwillingness to participate in the research or having a severe psychiatric disorder”.
The first step was to obtain permission from the original author. After that, The NSCB-S was translated from English into Persian by two psychology professors. Next, it was back-translated by two bilingual mental health professionals at Kermanshah University of Medical Sciences. The final version was reviewed for clarity and cultural appropriateness. In the next step, the scale was piloted with 30 overweight and obese and individuals at Kermanshah Nutrition Clinics to ensure the items were comprehensible. Participants completed the NSCB-S, the Physical Appearance Perfectionism Scale, the Positive and Negative Affect Scale, the Self-Compassion Scale, the Fear of Compassion Scale, and the Self-Criticism Scale.
This study was approved by Research Ethics Committees of Kermanshah Razi University under the ethical approval code No. IR.RAZI.REC.1404.016. All participants provided informed consent and were assured of confidentiality, and they participated voluntarily.
Negative Self-Compassion Beliefs (NSCB-S): Chwyl et al. (2020) suggested the key Negative Self-Compassion Beliefs: (a) complacency, such as “I will become complacent if I accept my imperfections completely”, (b) self-indulgence, such as “If I’m kind toward my flaws, I won’t have the discipline needed to succeed”, and (c) less self-responsibility, such as “I’ll take less responsibility for my shortcomings if I don’t constantly criticize myself”. This scale is rated on a 5-point Likert scale (1= completely disagree to 5=strongly agree) [5]. Internal consistency of the NSCB-S was excellent (α=0.94) [31].
Physical Appearance Perfectionism (PAPS): This scale consists of 12 items and two factors -worry about imperfection, hope for perfection. Items are rated on a 5-point Likert scale. This scale demonstrated high reliability, as indicated by Cronbach’s alpha, in an Iranian population [34].
Self-Compassion (SCS-SF): This short form comprises 12 items, rated on a 5-point Likert from 1 (almost never) to 5 (almost always). It has shown a strong correlation with long form (r=0.97). It measures three bipolar components: self-kindness vs. self-judgment, mindfulness vs. over identification, and common humanity vs. isolation [35]. Prior research has supported the three- factor structure of SCS–SF with acceptable internal consistency of 0.78 In an Iranian sample [36].
Positive and Negative Affect (PANAS): It has been driven from the Positive and Negative Affect Scale (20-Item) proposed by Watson et al. [37]. The subscale includes 10 items, that scored on a 5-point from 1 to 5. The internal consistency for the Iranian sample was 0.77 [38].
Fear of Compassion: This scale was designed by Gilbert [30], that consists of 38 items and three subscales: fear of expressing compassion to other people, fear of receiving compassion from others, and fear of self‑compassion. Items were scored from 0 to 4. Cronbach’s alpha coefficients for the Iranian sample in the subscales of fear of expressing compassion to others, fear of responding to compassion from others, and fear of self‑compassion were α = 0.85, α = 0.95, and α = 0.96, respectively [39].
Self-Criticism: This scale was developed by Gilbert, and has 22 items [40]. It measures self-critical thoughts and emotions in undesired situations. Items are scored on a 5-point Likert from 0 to 4. Cronbach’s alpha coefficients for this measure were 90% in self-incompetence and self-hatred subscales [41]. The reliability coefficients were 0.89 for self-incompetency and 0.73 for self-hated in the Iranian sample [42]. In the present study, the self-criticism subscale was used.
Results
In this study, 207 overweight and obese individuals (149 women, 72%, and 58 men, 28%) aged 14 to 55 years with mean: 33.5 ± 10.22 participated. Of these, 126 (60/86(visited a nutritionist for the first time, and 81 (39/13) reported a prior history of visiting a nutritionist. All participants were fluent in Persian and had a BMI over 25 kg/m2. The mean score on the NSCB-S for the sample was 27.70. Table 1 displays Means and Standard Deviations of variables by Gender.
This quantitative study was performed with 207 overweight individuals who had referred to Kermanshah Nutrition Clinics between June and September 2025 (149 women, 72%, and 58 men, 28%). Following Klein’s (2010) recommendation for structural equation modelling, a sample size of at least 200 people is defensible [33]. Participants (n=207) were selected through convenience sampling from nutrition clinics. The sample consisted of overweight and obese individuals. Inclusion criteria were fluency in Persian and a body mass index (BMI) over 25 kg/m2. Exclusion criteria included “Unwillingness to participate in the research or having a severe psychiatric disorder”.
The first step was to obtain permission from the original author. After that, The NSCB-S was translated from English into Persian by two psychology professors. Next, it was back-translated by two bilingual mental health professionals at Kermanshah University of Medical Sciences. The final version was reviewed for clarity and cultural appropriateness. In the next step, the scale was piloted with 30 overweight and obese and individuals at Kermanshah Nutrition Clinics to ensure the items were comprehensible. Participants completed the NSCB-S, the Physical Appearance Perfectionism Scale, the Positive and Negative Affect Scale, the Self-Compassion Scale, the Fear of Compassion Scale, and the Self-Criticism Scale.
This study was approved by Research Ethics Committees of Kermanshah Razi University under the ethical approval code No. IR.RAZI.REC.1404.016. All participants provided informed consent and were assured of confidentiality, and they participated voluntarily.
Negative Self-Compassion Beliefs (NSCB-S): Chwyl et al. (2020) suggested the key Negative Self-Compassion Beliefs: (a) complacency, such as “I will become complacent if I accept my imperfections completely”, (b) self-indulgence, such as “If I’m kind toward my flaws, I won’t have the discipline needed to succeed”, and (c) less self-responsibility, such as “I’ll take less responsibility for my shortcomings if I don’t constantly criticize myself”. This scale is rated on a 5-point Likert scale (1= completely disagree to 5=strongly agree) [5]. Internal consistency of the NSCB-S was excellent (α=0.94) [31].
Physical Appearance Perfectionism (PAPS): This scale consists of 12 items and two factors -worry about imperfection, hope for perfection. Items are rated on a 5-point Likert scale. This scale demonstrated high reliability, as indicated by Cronbach’s alpha, in an Iranian population [34].
Self-Compassion (SCS-SF): This short form comprises 12 items, rated on a 5-point Likert from 1 (almost never) to 5 (almost always). It has shown a strong correlation with long form (r=0.97). It measures three bipolar components: self-kindness vs. self-judgment, mindfulness vs. over identification, and common humanity vs. isolation [35]. Prior research has supported the three- factor structure of SCS–SF with acceptable internal consistency of 0.78 In an Iranian sample [36].
Positive and Negative Affect (PANAS): It has been driven from the Positive and Negative Affect Scale (20-Item) proposed by Watson et al. [37]. The subscale includes 10 items, that scored on a 5-point from 1 to 5. The internal consistency for the Iranian sample was 0.77 [38].
Fear of Compassion: This scale was designed by Gilbert [30], that consists of 38 items and three subscales: fear of expressing compassion to other people, fear of receiving compassion from others, and fear of self‑compassion. Items were scored from 0 to 4. Cronbach’s alpha coefficients for the Iranian sample in the subscales of fear of expressing compassion to others, fear of responding to compassion from others, and fear of self‑compassion were α = 0.85, α = 0.95, and α = 0.96, respectively [39].
Self-Criticism: This scale was developed by Gilbert, and has 22 items [40]. It measures self-critical thoughts and emotions in undesired situations. Items are scored on a 5-point Likert from 0 to 4. Cronbach’s alpha coefficients for this measure were 90% in self-incompetence and self-hatred subscales [41]. The reliability coefficients were 0.89 for self-incompetency and 0.73 for self-hated in the Iranian sample [42]. In the present study, the self-criticism subscale was used.
Results
In this study, 207 overweight and obese individuals (149 women, 72%, and 58 men, 28%) aged 14 to 55 years with mean: 33.5 ± 10.22 participated. Of these, 126 (60/86(visited a nutritionist for the first time, and 81 (39/13) reported a prior history of visiting a nutritionist. All participants were fluent in Persian and had a BMI over 25 kg/m2. The mean score on the NSCB-S for the sample was 27.70. Table 1 displays Means and Standard Deviations of variables by Gender.
Table 1. Means and Standard Deviations of participants by Gender
| Variables | Women(M) | Women (s.d) | Men(M) | Men (s.d) | Total |
| Negative Self-Compassion Beliefs | 27.65 | 9.2 | 27.82 | 9.1 | 27.70 |
| Physical Appearance Perfectionism | 41.42 | 10.3 | 41 | 10.1 | 41.30 |
| Self- Compassion | 34.88 | 6.4 | 35.36 | 6.2 | 35.01 |
| Fear of Compassion | 19.44 | 12.2 | 21.93 | 12.5 | 20.14 |
| Self-Criticism | 22.65 | 13.9 | 21.72 | 13.3 | 22.39 |
| Negative Affect | 25.61 | 8.07 | 23.68 | 7.39 | 48.00 |
| Positive Affect | 30.18 | 7.92 | 33.12 | 7.6 | 50.00 |
The construct validity of this scale was assessed using structural equation modelling, and a single-factor model was estimated. GFI, CFI, AGFI, IFI, NFI, NNFI, REMSEA, RMR and X2 /df indices were measured. If the model is fitted, the CFI, NFI, NNFI, GFI, AGFI, and IFI indices are 0.90 or higher and the REMSEA indice is 0.08 or lower. in addition, the X2 /df should be less than 3. The Model fit indices confirm the suitability of the model (Table 2). Internal consistency of the NSCB-S was calculated using Cronbach’s alpha (α=0/93). Figure 1 displays Confirmatory factor analysis of the NSCB-S.
Table 2. Fit indices of the one factor model of the NSCB-S
| Fit indexes | X2 | P | X2/df | RMR | GFI | IFI | CFI | AGFI | NNFI | NFI | RMSEA | |
| NSCB-S | 79.26 | 0.001 | 2.26 | .036 | .93 | .99 | .99 | .89 | .98 | .98 | .078 |
Figure1. Confirmatory factor analysis of the NSCB-S
Table 3. Convergent and Divergent Validity of Negative Self-Compassion Beliefs scale
| 7 | 6 | 5 | 4 | 3 | 2 | 1 | Variables | ||
| 1 | Negative Self-Compassion Beliefs | ||||||||
| 1 | 0/23** | Physical Appearance Perfectionism | |||||||
| 1 | -0/16* | -0/25* | Self-Compassion | ||||||
| 1 | -0/13* | 0/25** | 0/51** | Fear of Compassion | |||||
| 1 | 0/57** | -0/19** | 0/33** | 0/40** | Self-Criticism | ||||
| 1 | 0/53** | 0/32** | -0/16* | 0/14* | 0/32** | Negative Affect | |||
| 1 | -0/26** | -0/36** | -0/30** | 0/19** | 0/16* | -0/21* | Positive Affect | ||
Divergent and convergent validity of the NSCB-S were assessed using the Physical Appearance Perfectionism Scale, the Positive and Negative Affect Scale, the Self-Compassion Scale, the Fear of Compassion Scales and the Self-Criticism Scale. Table 3 shows that NSCB-S was positively correlated with physical appearance perfectionism (r=0.23, p=0.001), fear of compassion (r=0.51, p=0.001), self-criticism (r=0.40, p=0.000), and negative affect (r=0.32, p=0.000), supporting convergent validity. In contrast, the NSCB-S was negatively and significantly correlated with Self-Compassion (r=-0.25, p=0.000) and Positive Affect (r=-0.21, p=0.042), indicating adequate divergent validity.
Discussion
Overweight individuals encounter internal and external barriers to self-compassion [43]. Negative self-compassion beliefs represent one such barriers. The present study examined the psychometric properties of NSCB-S (Persian version) in overweight and obese individuals. The findings of confirmatory factor analysis confirmed the one factor model of this scale. Results are in the line with the findings of an original study [31], which also reported that a single factor model has a good fit. Although, the scale was initially conceptualised as comprising three factors, based on the earlier works by Gilbert et al. (2011) and Neff and Germer (2013) [30, 44], the empirical results of that original study and the present research support a unidimensional (single-factor) model.
First, in explaining these findings, it can be argued that individuals who hold negative beliefs of self-compassion are also likely to endorse other maladaptive beliefs. Moreover, the three factors identified in this scale (complacency, self-indulgence, and less self-responsibility), appear to share a common theme: a fear of lack of motivation and failing to take action. Second, as Neff and Germer (2018) have suggested two aspects of self-compassion: Yin and Yang. Many people mistakenly equate self-compassion with surrendering to circumstances and believe that it eliminates the need for self-correction or purposeful action. Some assume that self-compassion involves only self-acceptance (Yin) without realizing that compassion involves taking constructive action (Yang) [29]. In fact, some overweight individuals express that behaving compassionately may interfere with their motivation to improve themselves, hinder weight lose efforts, and undermine personal responsibility during emotionally challenging situations.
Third, Neff and Germer (2019) argue that common misunderstandings about the meaning and consequences of self-compassion are a primary reason why people hold negative beliefs about it. Selfishness, self-pity, always being nice, and self-indulgence are common misconceptions about self-compassion [45]. Accordingly, it appears that these three factors share a common underlying feature, which justifies modelling them as a single factor.
In addition, findings revealed that negative self-compassion beliefs have a positive significant corelation with perfectionism about appearance, fear of compassion, self-criticism and negative affect. Inverse association between perfectionism and negative affect with self-compassion have been previously documented [43,46,47]. Furthermore, fear of self-compassion scale has a positive correlation with negative self-compassion beliefs, which indicates a suitable divergent validity. It is in line with findings by Chwyl (2021) [31], which reported a significant negative relationship between the NBSC-S and self-compassion. It also aligns with Gilbert’s (2011) work, which showed that fear of compassion is positively correlated with self-blame, anxiety, stress, and depression [30]. This finding is consistent with results by Khanjani (2020), which similarly demonstrated significant positive relationship between fear of compassion, anxiety, stress, and depression [39]. Taken together, fear of self-compassion and negative beliefs about it reflect a negative attitude toward self-compassion, which may be associated with more negative attitudes toward overeating, especially after an unsuccessful diet [20]. Conceptually, fear of self-compassion primarily reflects affective barriers, whereas negative self-compassion beliefs more directly reflect underlying cognitive appraisals.
This study has the following limitations: firstly, the reliance on convenience sampling restricts its applicability to other populations and general public, such as children and adults. Therefore, future studies should focus on validating this scale within other populations, such as adolescents, individuals with eating disorders, or culturally diverse groups.
Discussion
Overweight individuals encounter internal and external barriers to self-compassion [43]. Negative self-compassion beliefs represent one such barriers. The present study examined the psychometric properties of NSCB-S (Persian version) in overweight and obese individuals. The findings of confirmatory factor analysis confirmed the one factor model of this scale. Results are in the line with the findings of an original study [31], which also reported that a single factor model has a good fit. Although, the scale was initially conceptualised as comprising three factors, based on the earlier works by Gilbert et al. (2011) and Neff and Germer (2013) [30, 44], the empirical results of that original study and the present research support a unidimensional (single-factor) model.
First, in explaining these findings, it can be argued that individuals who hold negative beliefs of self-compassion are also likely to endorse other maladaptive beliefs. Moreover, the three factors identified in this scale (complacency, self-indulgence, and less self-responsibility), appear to share a common theme: a fear of lack of motivation and failing to take action. Second, as Neff and Germer (2018) have suggested two aspects of self-compassion: Yin and Yang. Many people mistakenly equate self-compassion with surrendering to circumstances and believe that it eliminates the need for self-correction or purposeful action. Some assume that self-compassion involves only self-acceptance (Yin) without realizing that compassion involves taking constructive action (Yang) [29]. In fact, some overweight individuals express that behaving compassionately may interfere with their motivation to improve themselves, hinder weight lose efforts, and undermine personal responsibility during emotionally challenging situations.
Third, Neff and Germer (2019) argue that common misunderstandings about the meaning and consequences of self-compassion are a primary reason why people hold negative beliefs about it. Selfishness, self-pity, always being nice, and self-indulgence are common misconceptions about self-compassion [45]. Accordingly, it appears that these three factors share a common underlying feature, which justifies modelling them as a single factor.
In addition, findings revealed that negative self-compassion beliefs have a positive significant corelation with perfectionism about appearance, fear of compassion, self-criticism and negative affect. Inverse association between perfectionism and negative affect with self-compassion have been previously documented [43,46,47]. Furthermore, fear of self-compassion scale has a positive correlation with negative self-compassion beliefs, which indicates a suitable divergent validity. It is in line with findings by Chwyl (2021) [31], which reported a significant negative relationship between the NBSC-S and self-compassion. It also aligns with Gilbert’s (2011) work, which showed that fear of compassion is positively correlated with self-blame, anxiety, stress, and depression [30]. This finding is consistent with results by Khanjani (2020), which similarly demonstrated significant positive relationship between fear of compassion, anxiety, stress, and depression [39]. Taken together, fear of self-compassion and negative beliefs about it reflect a negative attitude toward self-compassion, which may be associated with more negative attitudes toward overeating, especially after an unsuccessful diet [20]. Conceptually, fear of self-compassion primarily reflects affective barriers, whereas negative self-compassion beliefs more directly reflect underlying cognitive appraisals.
This study has the following limitations: firstly, the reliance on convenience sampling restricts its applicability to other populations and general public, such as children and adults. Therefore, future studies should focus on validating this scale within other populations, such as adolescents, individuals with eating disorders, or culturally diverse groups.
Overall, the current study aimed to validate the NSCB-S among overweight and obese individuals seeking weight loss through community-based approaches. The results 0f confirmatory factor analysis demonstrated that NSCB-S had good psychometric properties and can be used in future research.
References
- Santos I, Sniehotta FF, Marques MM, Carraça EV, Teixeira PJ. Prevalence of personal weight control attempts in adults: a systematic review and meta-analysis. Obes Rev. 2017;18(1):32-50. [DOI: 10.1111/obr.12466] [PMID] [PMCID]
- Neff K. Self-compassion: an alternative conceptualization of a healthy attitude toward oneself. Self identity. 2003;2(2):85-101. [DOI: 10.1080/15298860309032]
- Dulloo AG, Montani JP. Pathways from dieting to weight regain, to obesity and to the metabolic syndrome: an overview. Obes Rev. 2015;16 Suppl 1:1-6. [DOI: 10.1111/obr.12250] [PMID]
- Kirk SFL, Price SL, Penney TL, Rehman L, Lyons RF, Piccinini-Vallis H, et al. Blame, shame, and lack of support: a multilevel study on obesity management. Qual Health Res. 2014;24(6):790-800. [DOI: 10.1177/1049732314529667] [PMID]
- Sikorski C, Luppa M, Brähler E, König HH, Riedel-Heller SG. Obese children, adults and senior citizens in the eyes of the general public: results of a representative study on stigma and causation of obesity. Plos One. 2012;7(10):e46924. [DOI: 10.1371/journal.pone.0046924] [PMID] [PMCID]
- Puhl RM, Heuer CA. The stigma of obesity: a review and update. Obes. 2009;17(5):941-64. [DOI: 10.1038/oby.2008.636] [PMID]
- Vallis M. Quality of life and psychological well-being in obesity management: improving the odds of success by managing distress. Int J Clin Pract. 2016;70(3):196-205. [DOI: 10.1111/ijcp.12765] [PMID] [PMCID]
- Rahimi-Ardabili H, Reynolds R, Vartanian LR, McLeod LVD, Zwar N. A Systematic review of the efficacy of interventions that aim to increase self-compassion on nutrition habits, eating behaviours, body weight and body image. Mindfulness. 2018;9(2):388-400. [DOI: 10.1007/s12671-017-0804-0]
- Thøgersen-Ntoumani C, Dodos LA, Stenling A, Ntoumanis N. Does self-compassion help to deal with dietary lapses among overweight and obese adults who pursue weight-loss goals? Br J Health Psychol. 2021;26(3):767-88. [DOI: 10.1111/bjhp.12499] [PMID] [PMCID]
- Wasylkiw L, MacKinnon AL, MacLellan AM. Exploring the link between self-compassion and body image in university women. Body Image. 2012;9(2):236-45. [DOI: 10.1016/j.bodyim.2012.01.007] [PMID]
- Marta-Simões J, Ferreira C, Mendes AL. Exploring the effect of external shame on body appreciation among Portuguese young adults: the role of self-compassion. Eat Behav. 2016;23:174-9. [DOI: 10.1016/j.eatbeh.2016.10.006] [PMID]
- Pinto-Gouveia J, Duarte C, Matos M, Fráguas S. The protective role of self-compassion in relation to psychopathology symptoms and quality of life in chronic and in cancer patients. Clin Psychol Psychother. 2014;21(4):311-23. [DOI: 10.1002/cpp.1838] [PMID]
- Ferreira C, Pinto-Gouveia J, Duarte C. Self-compassion in the face of shame and body image dissatisfaction: implications for eating disorders. Eat Behav. 2013;14(2):207-10. [DOI: 10.1016/j.eatbeh.2013.01.005] [PMID]
- Ferreira C, Matos M, Duarte C, Pinto-Gouveia J. Shame memories and eating psychopathology: the buffering effect of self-compassion. Eur Eat Disord Rev. 2014;22(6):487-94. [DOI: 10.1002/erv.2322] [PMID]
- Duarte C, Pinto-Gouveia J, Ferreira C, Batista D. Body image as a source of shame: a new measure for the assessment of the multifaceted nature of body image shame. Clin Psychol Psychother. 2015;22(6):656-66. [DOI: 10.1002/cpp.1925] [PMID]
- Kelly AC, Vimalakanthan K, Carter JC. Understanding the roles of self-esteem, self-compassion, and fear of self-compassion in eating disorder pathology: an examination of female students and eating disorder patients. Eat Behav. 2014;15(3):388-91. [DOI: 10.1016/j.eatbeh.2014.04.008] [PMID]
- Germer CK, Neff KD. Self-compassion in clinical practice. J Clin Psychol. 2013;69(8):856-67. [DOI: 10.1002/jclp.22021] [PMID]
- Leary MR, Tate EB, Adams CE, Allen AB, Hancock J. Self-compassion and reactions to unpleasant self-relevant events: the implications of treating oneself kindly. J Pers Soc Psychol. 2007;92(5):887-904. [DOI: 10.1037/0022-3514.92.5.887] [PMID]
- Breines JG, Chen S. Self-compassion increases self-improvement motivation. Pers Soc Psychol Bull. 2012;38(9):1133-43. [DOI: 10.1177/0146167212445599] [PMID]
- Adams CE, Leary MR. Promoting self-compassionate attitudes toward eating among restrictive and guilty eaters. J Social Clin Psychol. 2007;26(10):1120-44. [DOI: 10.1521/jscp.2007.26.10.1120]
- Hilbert A, Braehler E, Schmidt R, Löwe B, Häuser W, Zenger M. Self-Compassion as a resource in the self-stigma process of overweight and obese individuals. Obes Facts. 2015;8(5):293-301. [DOI: 10.1159/000438681] [PMID] [PMCID]
- Webb JB, Forman MJ. Evaluating the indirect effect of self-compassion on binge eating severity through cognitive-affective self-regulatory pathways. Eat Behav. 2013;14(2):224-8. [DOI: 10.1016/j.eatbeh.2012.12.005] [PMID]
- Palmeira L, Pinto-Gouveia J, Cunha M. The role of self-disgust in eating psychopathology in overweight and obesity: can self-compassion be useful? J Health Psychol. 2019;24(13):1807-16. [DOI: 10.1177/1359105317702212] [PMID]
- Gilbert P, McEwan K, Catarino F, Baião R, Palmeira L. Fears of happiness and compassion in relationship with depression, alexithymia, and attachment security in a depressed sample. Br J Clin Psychol. 2014;53(2):228-44. [DOI: 10.1111/bjc.12037] [PMID]
- Rockliff H, Gilbert P, McEwan K, Lightman S, Glover D. A pilot exploration of heart rate variability and salivary cortisol responses to compassion-focused imagery. J Treat Evaluation. 2008. [LINK]
- Gilbert P, Procter S. Compassionate mind training for people with high shame and self‐criticism: overview and pilot study of a group therapy approach. Clin Psychol Psycho Int J Theory Pract. 2006;13(6):353-79. [DOI: 10.1002/cpp.507]
- Gilbert P, Baldwin MW, Irons C, Baccus JR, Palmer M. Self-criticism and self-warmth: an imagery study exploring their relation to depression. J Cognitive Psychother. 2006;20(2):183. [DOI: 10.1891/088983906780639817]
- Germer C, Neff K. Mindful self-compassion (MSC). InHandbook of mindfulness-based programmes. 2019;357-367. [LINK]
- Neff K, Germer C. The mindful self-compassion workbook: a proven way to accept yourself, build inner strength, and thriveÿ ÿ. Guilford Publications. 2018. [LINK]
- Gilbert P, McEwan K, Matos M, Rivis A. Fears of compassion: development of three self-report measures. Psychol Psychother. 2011;84(3):239-55. [DOI: 10.1348/147608310X526511] [PMID]
- Chwyl C, Chen P, Zaki J. Beliefs about self-compassion: implications for coping and self-improvement. Pers Soc Psychol Bull. 2021;47(9):1327-42. [DOI: 10.1177/0146167220965303] [PMID]
- Brenton-Peters J, Consedine NS, Boggiss A, Wallace-Boyd K, Roy R, Serlachius A. Self-compassion in weight management: a systematic review. J Psychosom Res. 2021;150:110617. [DOI: 10.1016/j.jpsychores.2021.110617] [PMID]
- Kline RB. Principles and practice of structural equation modeling (3rd ed.): new york: guilford press. 2023. [LINK]
- Yang H, Stoeber J. The physical appearance perfectionism scale: development and preliminary validation. J Psychopathol Behav Assessment. 2012;34:69-83. [LINK]
- Raes F, Pommier E, Neff KD, Van Gucht D. Construction and factorial validation of a short form of the Self-Compassion Scale. Clin Psychol Psychother. 2011;18(3):250-5. [DOI: 10.1002/cpp.702] [PMID]
- Khanjani S, Foroughi AA, Sadghi K, Bahrainian SA. Psychometric properties of Iranian version of self-compassionscale (short form). Pajoohande. 2016;21(5):282-9. [LINK]
- Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54(6):1063-70. [DOI: 10.1037//0022-3514.54.6.1063] [PMID]
- SHARIFI HP, Bashardoust S, EMAMI PS. Psychometric properties of positive and negative affect (Panas). J Psychol Res. 2012;4(13):17-27. [Persian] [LINK]
- Khanjani S, Foroughi AA, Tahmasebi A, Bavafa A, Jaberghaderi N, Rafiee S. Factorial structure and construct validity of an Iranian version of the fear of compassion scale: a study in nurses. Iran J Nurs Midwifery Res. 2020;25(6):490-6. [DOI: 10.4103/ijnmr.IJNMR_151_19] [PMID] [PMCID]
- Gilbert P, Clarke M, Hempel S, Miles JN, Irons C. Forms of self-criticizing/attacking and self-reassuring scale. British J Clin Psychol. 2004. [DOI: 10.1037/t54209-000]
- Gilbert P, Clarke M, Hempel S, Miles JN, Irons C. Criticizing and reassuring oneself: an exploration of forms, styles and reasons in female students. Br J Clin Psychol. 2004;43(Pt 1):31-50. [DOI: 10.1348/014466504772812959] [PMID]
- Ghahremani OM, Mohammadkhani P, Hatami M, Mohammadrezaei R. Investigating the psychometric properties of self-criticism and self-reassurance scale in Iranian Students. 2020;8(1):65-72. [DOI: 10.32598/jpcp.8.1.67]
- Jeziorek A, Riazi A. Experiences of barriers to self-compassion in women experiencing weight difficulties: an interpretative phenomenological analysis. J Pers Med. 2022;12(9):1504. [DOI: 10.3390/jpm12091504] [PMID] [PMCID]
- Neff KD, Germer CK. A pilot study and randomized controlled trial of the mindful self-compassion program. J Clin Psychol. 2013;69(1):28-44. [DOI: 10.1002/jclp.21923] [PMID]
- Germer C, Neff K. Mindful self-compassion (MSC). InHandbook of mindfulness-based programme. 2019:357-67. [LINK]
- Barnett MD, Sharp KJ. Maladaptive perfectionism, body image satisfaction, and disordered eating behaviors among U.S. college women: the mediating role of self-compassion. Personal Individual Differences. 2016;99:225-34. [DOI: 10.1016/j.paid.2016.05.004]
- Foroughi A, Khanjani S, Mousavi Asl E. Relationship of concern about body dysmorphia with external shame, perfectionism, and negative affect: the mediating role of self-compassion. Iran J Psychiatry Behav Sci. 2019;13(2):e80186. [DOI: 10.5812/ijpbs.80186]
Article Type: Research Article |
Subject:
Clinical Psychology
Received: 2025/07/30 | Accepted: 2025/09/20 | Published: 2025/09/25
Received: 2025/07/30 | Accepted: 2025/09/20 | Published: 2025/09/25
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Hamadan University of Medical Sciences.
Published by UMSHA Press
Journal Tel: +989025126654
Publisher Tel: +985136014377
Website: http://ajnpp.umsha.ac.ir
Email: avicennajnpp[at]gmail.com
