

Volume 10, Issue 1 (February 2023)
Avicenna J Neuro Psycho Physiology 2023, 10(1): 8-14 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mirzaei-Alavijeh M, Fatahi H, Jalilian F. Psychometric of Water Intake Questionnaire in Patients with Kidney Stones: Investigation of Socio-Cognitive Determinants. Avicenna J Neuro Psycho Physiology 2023; 10 (1) :8-14
URL: http://ajnpp.umsha.ac.ir/article-1-446-en.html
URL: http://ajnpp.umsha.ac.ir/article-1-446-en.html



1- Social Development and Health Promotion Research Center, Health Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran
2- Department of Health Education and Promotion, School of Health, Kermanshah University of Medical Sciences, Kermanshah, Iran
3- Social Development and Health Promotion Research Center, Health Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran ,f_jalilian@yahoo.com
2- Department of Health Education and Promotion, School of Health, Kermanshah University of Medical Sciences, Kermanshah, Iran
3- Social Development and Health Promotion Research Center, Health Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran ,
Full-Text [PDF 1675 kb]
(708 Downloads)
| Abstract (HTML) (3202 Views)
Table 2. Items Deleted in CIA
Table 3. Evaluation of ICC (Test-retest study)
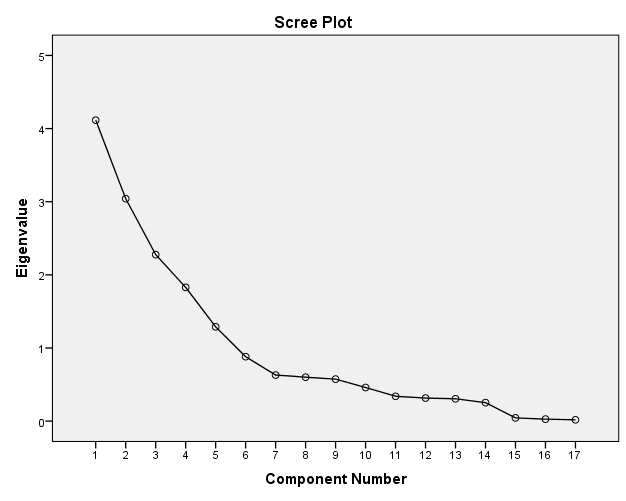
Figure 1. Scree plot of the structures studied among the participants
Discussion
The current study aimed to determine the psychometric evaluation of socio-cognitive determinants of the water intake questionnaire among patients with kidney stones. The obtained finding suggested that the socio-cognitive determinants of the water intake questionnaire were found to have acceptable internal consistency (Cronbach alpha of determinants between 0.65-0.85), and the theoretical assumptions for face, content, and construct validities were confirmed. Furthermore, the ICC of socio-cognitive determinants was high (ICC between 0.810 - 0.911). This finding is similar to the results reported by other studies. For instance, Lindberg and Fernandes carried out research on 113 Portuguese hemodialysis patients with the aim of assessing fluid intake appraisal inventory and indicated that psychometric evaluation of the questionnaire is acceptable [17]. As well, Arya et al. indicated that their questionnaire for measuring fluid intake, output, behavior, and urinary symptoms is valid and reliable [18]. In addition, Crary et al. carried out the study with the aim of psychometric analysis of a functional oral intake questionnaire for stroke patients and denoted that this questionnaire had adequate reliability, validity, and sensitivity to change in functional oral intake [23]. Our findings suggested that our questionnaire has adequate reliability and validity.
Known-group validity also pinpointed that patients who consumed 2 liters or more of water per day had significantly higher self-efficacy and lower perceived barriers. In line with the present study, Gordon et al. stated that the perceived barrier was an important determinant in fluid intake among patients with kidney stones [24]. An important strategy to increase fluid intake is fluid intake when they do not feel thirsty. Moreover, McCauley et al., in their study, categorized major barriers to fluid intake into three general categories, including (a) not knowing the benefits of fluid intake, (b) disliking the taste of water and lack of thirst, and (c) need to void frequently [15]. Furthermore, Tarplin et al. demonstrated that patients successful at fluid intake were less likely to report the barriers [25]. In addition, self-efficacy is one of the determinants for a better understanding of how patients with kidney stones adhere to fluid intake [15]. Tarplin et al. indicated that only 32.7% of patients reported being very successful with their fluid intake [25]. It seems that tailoring education to an individual's specific barriers and self-efficacy to change behavior could increase their chance of success.
Leung et al., in their study, stated that having valid and reliable tools is a necessity for developing effective theory-based health promotion programs [26]. Our questionnaire could be used to predict or explain water intake behavior in order to develop programs to increase water intake behavior among patients with kidney stones. A marked advantage of using this tool is that the obtained information can be used in clinical practice to tailor intervention programs for patients with kidney stones.
The findings of this study pointed out that the mean score of perceived severity among female patients was significantly lower than that in male patients. Other determinants did not show significant statistical gender differences. Several studies illustrated that perceived severity was an important factor that predicts behavior [27, 28]. Our findings also indicated that patients with a good daily intake of water (2 liters and more) reported higher perceived severity compared to the poor water intake group (lower than 2 liters). Based on this finding, it seems that educational interventions are needed to improve perceived severity, especially among female patients.
Our findings indicated that only 9% of patients reported two or more liters of water intake during the day. In this regard, Gordon et al., in their study reported that the majority of patients (about 60%) were unsuccessful in fluid intake [24]. Increased fluid intake has been proposed as an inexpensive strategy to prevent kidney stones [29]. The comparison between the findings of the present research and those obtained in similar studies conducted abroad illustrated that the water intake is much lower among Iranian patients with kidney stones compared to those in developing countries. These findings can be a warning to health policymakers in Iran and should be the focus of special attention. These results pointed to the necessity of providing training on the easiest way to prevent relapse among Iranian patients with kidney stones (more than two liters per day).
The present study has some limitations. Firstly, our sample included patients with kidney stones in the west of Iran, and representatives of other populations were not available in the current study. Secondly, according to the non-probability of data collection, our findings maybe not be generalized to other groups of patients with kidney stones. Thirdly, the failure to evaluate the external validity of the questionnaire was another limitation of our study. Future studies are necessary to evaluate the external validity of this questionnaire. Finally, another limitation of the present study was the lack of attention to the threshold of thirst.
Conclusions
Moussa and Chakra, in their study among patients with kidney or ureteral stones in Beirut, reported that most patients were not receiving kidney stone prevention counseling [30]. Urologists and clinical nurses play a critical role in advice for patients' prevention of kidney stones. In addition, designing an evidence-based intervention for patients with kidney stones in order to increase their water intake is important. The current provided significant information for health planning programmers to develop water intake promotion programs among patients with kidney stones. In other words, the use of our scale may be useful for guiding implementers to evaluate the determinants related to water intake and the development of effective health promotion programs among Iranian patients with kidney stones. In general, it was found that using the current questionnaire helps us to identify the predictors of low water intake in patients with kidney stones. A thorough understanding of the problems posed to water intake can be helpful in focusing interventions for patients with kidney stones. Finally, the validity and reliability of the instrument proposed for the cognitive constructs are adequate to support the use of this questionnaire in research on the prediction of water intake among Iranian patients with kidney stones.
Abbreviations
Compliance with ethical guidelines
The Research Ethics Committee at Deputy of Research of the Kermanshah University of Medical Sciences in the west of Iran approved the study protocol (KUMS.REC.1397.045). Furthermore, the participants were provided with the participant information statement and signed the written consent form. Individual personal information was kept confidential.
Acknowledgments
The authors would like to thank Kermanshah University of Medical Sciences, Kermanshah, Iran. Furthermore, we sincerely thank all patients participating in the study for their cooperation.
Authorsʼ contributions
MMA and FJ contributed to the conception and design of the research; HF, MMA, and FJ contributed to the acquisition design; FJ contributed to the analysis and interpretation of the data. MMA contributed to the scientific edit. All authors approved the final manuscript.
Funding/Support
This study was funded by the Kermanshah University of Medical Sciences, Kermanshah, Iran (research number: 97191). The funding organizations had no role in the design of the study, collection, analysis, and interpretation of data and in writing the manuscript.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
1. López M, Hoppe B. History, epidemiology and regional diversities of urolithiasis. Pediatric Nephrology. 2010; 25(1):49-59. [DOI:10.1007/s00467-008-0960-5] [PMID] [PMCID]
2. Mikawlrawng K, Kumar S, Vandana R. Current scenario of urolithiasis and the use of medicinal plants as antiurolithiatic agents in Manipur (North East India): a review. International Journal of herbal Medicine. 2014; 2(1):1-12.
3. Coe FL, Evan A, Worcester E. Kidney stone disease. The Journal of Clinical Investigation. 2005; 115(10):2598-608. [DOI:10.1172/JCI26662] [PMID] [PMCID]
4. Rule AD, Roger VL, Melton LJ, Bergstralh EJ, Li X, Peyser PA, et al. Kidney stones associate with increased risk for myocardial infarction. Journal of the American Society of Nephrology. 2010; 21(10):1641-4. [DOI:10.1681/ASN.2010030253] [PMID] [PMCID]
5. Chauhan CK, Joshi MJ, Vaidya AD. Growth inhibition of struvite crystals in the presence of herbal extract Commiphora wightii. Journal of Materials Science: Materials in Medicine. 2009; 20(1):85-92. [DOI:10.1007/s10856-008-3489-z] [PMID]
6. Safarinejad MR. Adult urolithiasis in a population-based study in Iran: prevalence, incidence, and associated risk factors. Urological Research. 2007; 35(2):73-82. [DOI:10.1007/s00240-007-0084-6] [PMID]
7. Edvardsson VO, Indridason OS, Haraldsson G, Kjartansson O, Palsson R. Temporal trends in the incidence of kidney stone disease. Kidney International. 2013; 83(1):146-52. [DOI:10.1038/ki.2012.320] [PMID]
8. Dhanalakshmi S, Gayathri R, Vishnupriya V. Correlation between inadequate intake of water and prevalence of Renal Calculi–A survey. Journal of Pharmaceutical Sciences and Research. 2017; 9(4):429.
9. Pearle MS, Goldfarb DS, Assimos DG, Curhan G, Denu-Ciocca CJ, Matlaga BR, et al. Medical management of kidney stones: AUA guideline. The Journal of Urology. 2014; 192(2):316-24. [DOI:10.1016/j.juro.2014.05.006] [PMID]
10. Lotan Y, Buendia Jiménez I, Lenoir‐Wijnkoop I, Daudon M, Molinier L, Tack I, et al. Primary prevention of nephron-lithiasis is cost-effective for a national healthcare system. BJU International. 2012; 110(11):1060-7. [DOI:10.1111/j.1464-410X.2012.11212.x] [PMID]
11. Kok G, Gottlieb NH, Peters GJ, Mullen PD, Parcel GS, Ruiter RA, et al. A taxonomy of behaviour change methods: an Intervention Mapping approach. Health Psychology Review. 2016; 10(3):297-312. [DOI:10.1080/17437199.2015.1077155] [PMID] [PMCD]
12. Borghi L, Schianchi T, Meschi T, Guerra A, Allegri F, Maggiore U, et al. Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria. New England Journal of Medicine. 2002; 346(2):77-84. [DOI:10.1056/NEJMoa010369] [PMID]
13. O'Connor SM, Jardine AG, Millar K. The prediction of self-care behaviors in end-stage renal disease patients using Leventhal's Self-Regulatory Model. Journal of Psychosomatic Research. 2008; 65(2):191-200. [DOI:10.1016/j.jpsychores..02.008] [PMID]
14. Rich A, Brandes K, Mullan B, Hagger MS. Theory of planned behavior and adherence in chronic illness: a meta-analysis. Journal of Behavioral Medicine. 2015; 38(4):673-88. [DOI:10.1007/s10865-015-9644-3] [PMID]
15. McCauley LR, Dyer AJ, Stern K, Hicks T, Nguyen MM. Factors influencing fluid intake behavior among kidney stone formers. The Journal of Urology. 2012; 187(4):1282-6. [DOI:10.1016/j.juro.2011.11.111] [PMID]
16. Khalil A, Abdalrahim M. Knowledge, attitudes, and practices towards prevention and early detection of chronic kidney disease. International Nursing Review. 2014; 61(2):237-45. [DOI:10.1111/inr.12085] [PMID]
17. Lindberg M, Fernandes MA. Self-efficacy in relation to limited fluid intake amongst Portuguese haemodialysis patients. Journal of Renal Care. 2010; 36(3):133-8. [DOI:10.1111/j.1755-6686.2010.00182.x] [PMID]
18. Arya LA, Banks C, Gopal M, Northington GM. Development and testing of a new instrument to measure fluid intake, output, and urinary symptoms: the questionnaire-based voiding diary. American Journal of Obstetrics and Gynecology. 2008; 198(5):1-7. [DOI:10.1016/j.ajog.2008.01.049] [PMID]
19. Lindberg M, Wikström B, Lindberg P. Fluid Intake Appraisal Inventory: development and psychometric evaluation of a situation-specific measure for haemodialysis patients' self-efficacy to low fluid intake. Journal of Psychosomatic Research. 2007; 63(2):167-73. [DOI:10.1016/j.jpsychores.2007.03.013] [PMID]
20. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommend-ations. Research in Nursing & Health. 2007; 30(4):459-67. [DOI:10.1002/nur.20199] [PMID]
21. Lawshe CH. A quantitative approach to content validity. Personnel Psychology. 1975; 28(4):563-75. [DOI:10.1111/j.1744-6570.1975.tb01393.x]
22. Hayton JC, Allen DG, Scarpello V. Factor retention decisions in exploratory factor analysis: A tutorial on parallel analysis. Organizational Research Methods. 2004; 7(2):191-205. [DOI:10.1177/1094428104263675]
23. Crary MA, Mann GD, Groher ME. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Archives of Physical Medicine and Rehabilitation. 2005; 86(8):1516-20. [DOI:10.1016/j.apmr.2004.11.049] [PMID]
24. Gordon EJ, Prohaska TR, Gallant M, Siminoff LA. Self-care strategies and barriers among kidney transplant recipients: a qualitative study. Chronic Illness. 2009; 5(2):75-91. [DOI:10.1177/1742395309103558] [PMID]
25. Tarplin S, Monga M, Stern KL, McCauley LR, Sarkissian C, Nguyen MM. Predictors of reporting success with increased fluid intake among kidney stone patients. Urology. 2016; 88:49-56. [DOI:10.1016/j.urology.2015.10.024] [PMID]
26. Leung SF, Lee KL, Lee SM, Leung SC, Hung WS, Lee WL, et al. Psychometric properties of the SCOFF questionnaire (Chinese version) for screening eating disorders in Hong Kong secondary school students: A cross-sectional study. International Journal of Nursing Studies. 2009; 46(2):239-47. [DOI:10.1016/j.ijnurstu.2008.09.004] [PMID]
27. Ferrer RA, Klein WM, Avishai A, Jones K, Villegas M, Sheeran P. When does risk perception predict protection motivation for health threats? A person-by-situation analysis. PloS One. 2018; 13(3):e0191994. [DOI:10.1371/journal.pone.0191994] [PMID] [PMCID]
28. Nie R, Han Y, Xu J, Huang Q, Mao J. Illness perception, risk perception and health promotion self-care behaviors among Chinese patient with type 2 diabetes: A cross-sectional survey. Applied Nursing Research. 2018; 39:89-96. [DOI:10.1016/j.apnr.2017.11.010] [PMID]
29. Cheungpasitporn W, Rossetti S, Friend K, Erickson SB, Lieske JC. Treatment effect, adherence, and safety of high fluid intake for the prevention of incident and recurrent kidney stones: a systematic review and meta-analysis. Journal of Nephrology. 2016; 29(2):211-9. [DOI:10.1007/s40620-015-0210-4] [PMID] [PMCID]
30. Moussa M, Abou Chakra M. Patient's perception of kidney stone prevention within the emergency department and its adherence factors: a single institution study. BMC Emergency Medicine. 2019; 19(1):1-7. [DOI:10.1186/s12873-019-0263-0] [PMID] [PMCID]
Full-Text: (1034 Views)
Background
An unhealthy lifestyle (such as obesity and lack of physical activity) is linked to an increased kidney stone risk [1, 2]. Almost 80% of stones are composed of calcium oxalate (C2H2CaO5) and may be caused by infections, as well as environmental and metabolic factors [3]. Hematuria, blockage of urine flow, kidney colic, urinary tract infections, flank pain, and or nausea/vomiting are common symptoms of kidney stones [4]. Kidney stone is an increasing urological disorder affecting approximately 12% of the world's population [5]. Moreover, the kidney stones relapse rate was reported at 32% of cases after 5 years and 53% after 10 years [6]. The majority of the patients diagnosed with kidney stones are middle-aged, around 30-60 years old, and male (10%-20% versus 3-5% in females) [7]. Studies have indicated that daily water intake (in the recommended amount) is protective against kidney stones [8].
Based on the American Urological Association Medical Management of Kidney Stone Guidelines, stone former should have a minimum urine output of 2.5 L daily [9]. Increasing water intake is a cost-benefit prevention strategy for kidney stones; nonetheless, despite this simple prevention strategy, most patients do not intake adequate fluids [10]. Intervention programs should put and emphasise on socio-cognitive determinants that predict behaviors [11]. In water intake increasing programs, it would be useful to health educators to know how socio-cognitive related determinants, such as barriers, social norms, self-efficacy, attitude, or beliefs, are responsible for explaining behavior [12-14]. In summary, it is crucial to identify the cognitive determinants that may determine water intake among patients with kidney stones [15-19]. According to the absence of studies in developing countries, the present research aimed to assess the initial validity and reliability of socio-cognitive determinants of water intake questionnaire in a sample of patients with kidney stones in Iran.
Materials and Methods
Item Generation
The water intake questionnaire for patients with kidney stones was developed to evaluate cognitive determinants that explain water intake behavior among these patients. Items were at first generated according to the interviews with 38 patients with kidney stones and 12 experts, such as health educators and promoters, nephrology, health policymakers, health care management, nurses, and renal dieticians. Moreover, our item pool was developed from the questionnaires of socio-cognitive determinants related to water intake [15-19]. Interviews with patients with kidney stones and experts were collected by one MSc health education and promotion student in a face-to-face interview style (15-25 min). After explaining the aims of the study, the participants signed consent forms and were interviewed separately by the interviewer. In addition, the interviewers had been trained to ensure that the participants completely realized their words.
The socio-cognitive determinants related to the water intake included 23 items that measured the five constructs of 1) three items measured the perceived severity (e.g., "Inadequate water intake increases the probability of kidney stones relapse."). Four items measured the positive attitude towards water intake (e.g., "Water intake decreases the probability of kidney stones relapse."). Five items measured the subjective norms encouraging water intake (e.g., "My family encourages me to drink water"). Five items measured the self-efficacy towards water intake (e.g., "I am confident drink water before feeling thirsty."). Six items measured the perceived barriers (e.g., "I don't drink water if I don't feel thirsty."). In order to facilitate the subject's responses to the items, all items were scored based on a five-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree).
Validating the Questionnaire: Use of Face, Content, and Construct Validities
The validity of the questionnaire was evaluated by using face validity, content validity, and construct validity.
Face Validity
The qualitative method was used to evaluate face validity. In order to evaluate the face validity, a panel of 12 experts, consisting of health educators and promoters, nephrologists, health policymakers, health care management, and nurses, were face-to-face interviewed to approve the difficulty, relevancy, clarity, and ambiguity of the questionnaire. Comments from the expert group were taken, and minor modifications were made to some of the items based on expert opinions.
Content validity
Content Validity Ratio (CVR) and Content Validity Index (CVI) were used to evaluate content validity [20]. For this purpose, the questionnaire was administered to a panel of 12 experts, including six health educators, two health policymakers, two psychologists, and two urologists. The experts were asked to score each item by the following rankings as "completely necessary," "useful but unnecessary," and "unnecessary." The CVR was calculated using the "necessity" and "total item scores." To evaluate CVI, the experts were asked to answer the following question, "Did the items measure what they were intended to measure?" using a 4-point Likert scale in order to evaluate relevancy. The CVI value of each item was computed by dividing the number of experts who rated it as content valid (a ranking of 3 or 4) by the total number of experts. The total CVI value was calculated by dividing the sum of the "3" and "4" scores from each expert by the total number of experts. According to the Lawshe table, the minimum value for acceptable CVR and CVI were considered 0.62 and 0.79, respectively [21].
Construct Validity
To evaluate the construct validity, firstly, the Classical Item Analysis (CIA) was used. In the CIA method, the mean, standard deviation, and Corrected item-total Correlation (CITC) of each item were calculated. Secondly, the Exploratory Factor Analysis (EFA) with VARIMAX rotation using factor loadings of 0.40 was used to allocate items and determine the degree to which this factor structure replicated the original. The Kaiser-Meyer-Olkin (KMO) measured the sampling adequacy. The factorability of items was evaluated using the Bartlett test. A Scree plot was used to confirm the strengths of the exploratory agents. Likewise, to determine agents, the values that were equal to or greater than 1.3 were considered [22]. The EFA was evaluated by conducting a cross-sectional study of 115 patients with kidney stones in 2018. Participants were selected based on a convenience sampling method among patients with kidney stones who were referred to Imam Reza Hospital (IRH) in Kermanshah, the west of Iran. Only the subjects who were diagnosed with kidney stones were eligible to participate in the study. In addition, participants with incomplete personal or medical information and/or those who did not formally consent to participate were excluded. Among the 115 patients with kidney stones, 100 patients signed the consent form and voluntarily agreed to participate in our study. Therefore, the response rate was 86.9%.
Known-group validity
To evaluate the known-group validity of the questionnaire, the association between water intake status and socio-cognitive determinants was tested using an independent sample t-test (Table 5). The respondents were categorized into two water intake adherence groups based on their water intake per day: poor (lower than 2 liters) and good (2 liters and more).
Reliability
The reliability of the questionnaire was evaluated by examining its internal consistency via Cronbach's alpha. Considering Cronbach's alpha, a threshold of 0.70 was acceptable. Moreover, means and standard deviations (SD) were used for both the test-retest reproducibility between the two periods using the Intra-class Correlation Coefficient (ICC) with its 95% confidence interval. In order to evaluate ICC, 20 patients were randomly selected from the participants in the current study to perform a test-retest after two weeks.
Statistical Analysis
All data analysis was performed using the statistical package for social sciences (SPSS) (Version 20.0; IBM Corporation, Chicago, USA). A p-value of less than 0.05 was considered statistically significant.
Results
The mean age of respondents was 45.35 years [95% CI: 42.56, 48.13], ranging from 20-70 years. More details of the demographic characteristics of the participants are displayed in Table 1. The mean water intake of respondents was 930.01 cubic centimeters (cc) [95% CI: 804.96, 1055.03], ranging from 200-3000 cc. In addition, only 9% of participants reported they had two or more liters of water intake during the day.
Table 1. Distribution of the Demographic Characteristics among the Participants
The item impact method of all the sentences was more than 1.5, and therefore, none of the 23 items were omitted. Based on Lawshe's table, the acceptable lower limit for the CVR was considered 0.62, and for CVI, it was regarded as 0.79. Indicating content validity ratio and index for all items were acceptable. In the CIA method, it was found that one item from the attitude construct, three items from the attitude construct perceived barrier, one item from the perceived self-efficacy construct, and one item from the subjective norms construct had CITC less than 0.40 and was deleted (Table 2). Therefore, 18 finalized items were applied for the explanatory and confirmatory factor analysis.
The reliability of socio-cognitive determinants expressed in the Intra-class Correlation Coefficient is illustrated in Table 3.
Based on the American Urological Association Medical Management of Kidney Stone Guidelines, stone former should have a minimum urine output of 2.5 L daily [9]. Increasing water intake is a cost-benefit prevention strategy for kidney stones; nonetheless, despite this simple prevention strategy, most patients do not intake adequate fluids [10]. Intervention programs should put and emphasise on socio-cognitive determinants that predict behaviors [11]. In water intake increasing programs, it would be useful to health educators to know how socio-cognitive related determinants, such as barriers, social norms, self-efficacy, attitude, or beliefs, are responsible for explaining behavior [12-14]. In summary, it is crucial to identify the cognitive determinants that may determine water intake among patients with kidney stones [15-19]. According to the absence of studies in developing countries, the present research aimed to assess the initial validity and reliability of socio-cognitive determinants of water intake questionnaire in a sample of patients with kidney stones in Iran.
Materials and Methods
Item Generation
The water intake questionnaire for patients with kidney stones was developed to evaluate cognitive determinants that explain water intake behavior among these patients. Items were at first generated according to the interviews with 38 patients with kidney stones and 12 experts, such as health educators and promoters, nephrology, health policymakers, health care management, nurses, and renal dieticians. Moreover, our item pool was developed from the questionnaires of socio-cognitive determinants related to water intake [15-19]. Interviews with patients with kidney stones and experts were collected by one MSc health education and promotion student in a face-to-face interview style (15-25 min). After explaining the aims of the study, the participants signed consent forms and were interviewed separately by the interviewer. In addition, the interviewers had been trained to ensure that the participants completely realized their words.
The socio-cognitive determinants related to the water intake included 23 items that measured the five constructs of 1) three items measured the perceived severity (e.g., "Inadequate water intake increases the probability of kidney stones relapse."). Four items measured the positive attitude towards water intake (e.g., "Water intake decreases the probability of kidney stones relapse."). Five items measured the subjective norms encouraging water intake (e.g., "My family encourages me to drink water"). Five items measured the self-efficacy towards water intake (e.g., "I am confident drink water before feeling thirsty."). Six items measured the perceived barriers (e.g., "I don't drink water if I don't feel thirsty."). In order to facilitate the subject's responses to the items, all items were scored based on a five-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree).
Validating the Questionnaire: Use of Face, Content, and Construct Validities
The validity of the questionnaire was evaluated by using face validity, content validity, and construct validity.
Face Validity
The qualitative method was used to evaluate face validity. In order to evaluate the face validity, a panel of 12 experts, consisting of health educators and promoters, nephrologists, health policymakers, health care management, and nurses, were face-to-face interviewed to approve the difficulty, relevancy, clarity, and ambiguity of the questionnaire. Comments from the expert group were taken, and minor modifications were made to some of the items based on expert opinions.
Content validity
Content Validity Ratio (CVR) and Content Validity Index (CVI) were used to evaluate content validity [20]. For this purpose, the questionnaire was administered to a panel of 12 experts, including six health educators, two health policymakers, two psychologists, and two urologists. The experts were asked to score each item by the following rankings as "completely necessary," "useful but unnecessary," and "unnecessary." The CVR was calculated using the "necessity" and "total item scores." To evaluate CVI, the experts were asked to answer the following question, "Did the items measure what they were intended to measure?" using a 4-point Likert scale in order to evaluate relevancy. The CVI value of each item was computed by dividing the number of experts who rated it as content valid (a ranking of 3 or 4) by the total number of experts. The total CVI value was calculated by dividing the sum of the "3" and "4" scores from each expert by the total number of experts. According to the Lawshe table, the minimum value for acceptable CVR and CVI were considered 0.62 and 0.79, respectively [21].
Construct Validity
To evaluate the construct validity, firstly, the Classical Item Analysis (CIA) was used. In the CIA method, the mean, standard deviation, and Corrected item-total Correlation (CITC) of each item were calculated. Secondly, the Exploratory Factor Analysis (EFA) with VARIMAX rotation using factor loadings of 0.40 was used to allocate items and determine the degree to which this factor structure replicated the original. The Kaiser-Meyer-Olkin (KMO) measured the sampling adequacy. The factorability of items was evaluated using the Bartlett test. A Scree plot was used to confirm the strengths of the exploratory agents. Likewise, to determine agents, the values that were equal to or greater than 1.3 were considered [22]. The EFA was evaluated by conducting a cross-sectional study of 115 patients with kidney stones in 2018. Participants were selected based on a convenience sampling method among patients with kidney stones who were referred to Imam Reza Hospital (IRH) in Kermanshah, the west of Iran. Only the subjects who were diagnosed with kidney stones were eligible to participate in the study. In addition, participants with incomplete personal or medical information and/or those who did not formally consent to participate were excluded. Among the 115 patients with kidney stones, 100 patients signed the consent form and voluntarily agreed to participate in our study. Therefore, the response rate was 86.9%.
Known-group validity
To evaluate the known-group validity of the questionnaire, the association between water intake status and socio-cognitive determinants was tested using an independent sample t-test (Table 5). The respondents were categorized into two water intake adherence groups based on their water intake per day: poor (lower than 2 liters) and good (2 liters and more).
Reliability
The reliability of the questionnaire was evaluated by examining its internal consistency via Cronbach's alpha. Considering Cronbach's alpha, a threshold of 0.70 was acceptable. Moreover, means and standard deviations (SD) were used for both the test-retest reproducibility between the two periods using the Intra-class Correlation Coefficient (ICC) with its 95% confidence interval. In order to evaluate ICC, 20 patients were randomly selected from the participants in the current study to perform a test-retest after two weeks.
Statistical Analysis
All data analysis was performed using the statistical package for social sciences (SPSS) (Version 20.0; IBM Corporation, Chicago, USA). A p-value of less than 0.05 was considered statistically significant.
Results
The mean age of respondents was 45.35 years [95% CI: 42.56, 48.13], ranging from 20-70 years. More details of the demographic characteristics of the participants are displayed in Table 1. The mean water intake of respondents was 930.01 cubic centimeters (cc) [95% CI: 804.96, 1055.03], ranging from 200-3000 cc. In addition, only 9% of participants reported they had two or more liters of water intake during the day.
Table 1. Distribution of the Demographic Characteristics among the Participants
| Variables | Percent |
| Sex | |
| Female | 29 |
| Male | 71 |
| Marital status | |
| Married | 90 |
| Single | 10 |
| Education | |
| Illiterate | 21 |
| Primary school (1-6 grade) | 36 |
| High school (7-12 grade) | 21 |
| Academic (13-16 grade) | 22 |
| Economic status | |
| Independent | 65 |
| Dependent | 35 |
| Health insurance | |
| Yes | 88 |
| No | 12 |
| Location | |
| Urban | 74 |
| Rural | 26 |
The item impact method of all the sentences was more than 1.5, and therefore, none of the 23 items were omitted. Based on Lawshe's table, the acceptable lower limit for the CVR was considered 0.62, and for CVI, it was regarded as 0.79. Indicating content validity ratio and index for all items were acceptable. In the CIA method, it was found that one item from the attitude construct, three items from the attitude construct perceived barrier, one item from the perceived self-efficacy construct, and one item from the subjective norms construct had CITC less than 0.40 and was deleted (Table 2). Therefore, 18 finalized items were applied for the explanatory and confirmatory factor analysis.
The reliability of socio-cognitive determinants expressed in the Intra-class Correlation Coefficient is illustrated in Table 3.
Table 2. Items Deleted in CIA
| Reason of deleted | Construct | Item | No |
| CITC under 0.4 | Attitude | Water intake is beneficial in the prevention of kidney stone relapse. | 1 |
| CITC under 0.4 | Perceived Barrier | I'm not sure that the city water is healthy. | 2 |
| CITC under 0.4 | Perceived Barrier | Control of my urinary is more important than kidney stone disease. | 3 |
| CITC under 0.4 | Perceived Barrier | I do not like to water intake. | 4 |
| CITC under 0.4 | Subjective Norms | My friends encourage me to extra water intake. | 5 |
| CITC under 0.4 | Perceived Self-efficacy | I can ask my friends about the benefits of water intake. | 6 |
Table 3. Evaluation of ICC (Test-retest study)
| Constructs | ICC | 95% CI for ICC |
| Perceived Severity | 0.856 | 0.545-0.948 |
| Attitude | 0.883 | 0.729-0.952 |
| Subjective norm | 0.810 | 0.586-0.920 |
| Perceived self-efficacy | 0.911 | 0.793-0.964 |
| Perceived Barrier | 0.870 | 0.704-0.946 |
In addition, as displayed in Table 4, estimates of the reliability by using Cronbach's coefficient alpha and our result demonstrated the reliability coefficient for all cognitive variables suggested that the internal consistency was adequate. The 17 items were factor analyzed. The KMO test, which is the efficiency index of the sampling, was measured at 0.697. Bartlett's Test was also significant (P<0.001), suggesting the suitability of data for the factorial analysis. Based on Eigenvalues of ≥ 1.00 and factor loadings of ≥ 0.40, five factors were extracted, accounting for 73.83% of the variation. More details of exploratory factor analysis are depicted in Table 2. Furthermore, the scree plot diagram of factors is illustrated in Figure 1.
Figure 1. Scree plot of the structures studied among the participants
Table 4. Obtained Result of the Exploratory Factor Analysis
| 5 | 4 | 3 | 2 | 1 | Items | No |
| (4) Perceived Severity | ||||||
| 0.716 | Inadequate water intake increases the probability of kidney stones relapse. | 1 | ||||
| 0.710 | Inadequate water intake may lead to the chronic kidney diseases. | 2 | ||||
| 0.825 | Inadequate water intake increases the severity of my disease. | 3 | ||||
| (3) Attitude | ||||||
| 0.748 | Water intake decreases the probability of kidney stone relapse | 1 | ||||
| 0.828 | Water intake could be useful for the prevention of kidney stones. | 2 | ||||
| 0.868 | Water intake may control the complications of kidney stones. | 3 | ||||
| (5) Subjective norm | ||||||
| 0.790 | My family encourages me to water intake. | 1 | ||||
| 0.616 | Healthcare members encourage me to intake water. | 2 | ||||
| 0.654 | Other patients encourage me to water intake. | 3 | ||||
| 0.771 | Most people who are important to me think I should increase my water intake. | 4 | ||||
| (1) Perceived Self-efficacy | ||||||
| 0.810 | I am confident in drinking water before feeling thirsty. | 1 | ||||
| 0.977 | I am confident in consulting with my doctor about the benefit of water intake. | 2 | ||||
| 0.964 | I am confident in drinking water even if I do not desire it. | 3 | ||||
| 0.962 | I believe that I am confident daily drinking at least 2 L of water in order to prevent kidney stones. | 4 | ||||
| (2) Perceived Barrier | ||||||
| 0.687 | I forget to drink water, occasionally. | 1 | ||||
| 0.951 | I don't drink water if I don't feel thirsty. | 2 | ||||
| 0942 | I don't drink water at least 2 L daily because of the need to void frequently. | 3 | ||||
| 7.58 | 10.75 | 13.39 | 17.89 | 24.20 | Variance (%) | - |
| 73.83 | Total Variance | - | ||||
| 0.84 | 0.85 | 0.65 | 0.80 | 0.73 | Alpha coefficient of the structures | - |
Table 5. Known-group Validity of the Questionnaire and sex Differences in Socio-cognitive Determinants of Water Intake among the Participants
Finally, the results related to the known-group validity of the questionnaire and gender differences in socio-cognitive determinants of water intake among the participants are displayed in Table 5. | Perceived Severity | Attitude | Subjective norm | Perceived self-efficacy | Perceived Barrier | |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Known-group validity of the questionnaire | |||||
| Poor (lower than 2-liter) | 4.95 (2.38) | 13.66 (2.09) | 17.02 (3.53) | 8.37 (4.44) | 6.22 (3.88) |
| Good (2-liter and more) | 6.11 (3.37) | 13.44 (2.01) | 16.22 (5.19) | 13.66 (5.31) | 3.66 (1.65) |
| P-value | 0.186 | 0.761 | 0.537 | 0.001 | 0.002 |
| Differences in socio-cognitive determinants of water intake | |||||
| Women | 4.37 (1.69) | 13.96 (2.11) | 17.53 (4.01) | 8.41 (4.25) | 6.31 (3.86) |
| Men | 5.33 (2.70) | 13.51 (2.06) | 16.71 (3.55) | 9.02 (4.95) | 5.85 (3.79) |
| P-value | 0.036 | 0.328 | 0.323 | 0.560 | 0.592 |
Discussion
The current study aimed to determine the psychometric evaluation of socio-cognitive determinants of the water intake questionnaire among patients with kidney stones. The obtained finding suggested that the socio-cognitive determinants of the water intake questionnaire were found to have acceptable internal consistency (Cronbach alpha of determinants between 0.65-0.85), and the theoretical assumptions for face, content, and construct validities were confirmed. Furthermore, the ICC of socio-cognitive determinants was high (ICC between 0.810 - 0.911). This finding is similar to the results reported by other studies. For instance, Lindberg and Fernandes carried out research on 113 Portuguese hemodialysis patients with the aim of assessing fluid intake appraisal inventory and indicated that psychometric evaluation of the questionnaire is acceptable [17]. As well, Arya et al. indicated that their questionnaire for measuring fluid intake, output, behavior, and urinary symptoms is valid and reliable [18]. In addition, Crary et al. carried out the study with the aim of psychometric analysis of a functional oral intake questionnaire for stroke patients and denoted that this questionnaire had adequate reliability, validity, and sensitivity to change in functional oral intake [23]. Our findings suggested that our questionnaire has adequate reliability and validity.
Known-group validity also pinpointed that patients who consumed 2 liters or more of water per day had significantly higher self-efficacy and lower perceived barriers. In line with the present study, Gordon et al. stated that the perceived barrier was an important determinant in fluid intake among patients with kidney stones [24]. An important strategy to increase fluid intake is fluid intake when they do not feel thirsty. Moreover, McCauley et al., in their study, categorized major barriers to fluid intake into three general categories, including (a) not knowing the benefits of fluid intake, (b) disliking the taste of water and lack of thirst, and (c) need to void frequently [15]. Furthermore, Tarplin et al. demonstrated that patients successful at fluid intake were less likely to report the barriers [25]. In addition, self-efficacy is one of the determinants for a better understanding of how patients with kidney stones adhere to fluid intake [15]. Tarplin et al. indicated that only 32.7% of patients reported being very successful with their fluid intake [25]. It seems that tailoring education to an individual's specific barriers and self-efficacy to change behavior could increase their chance of success.
Leung et al., in their study, stated that having valid and reliable tools is a necessity for developing effective theory-based health promotion programs [26]. Our questionnaire could be used to predict or explain water intake behavior in order to develop programs to increase water intake behavior among patients with kidney stones. A marked advantage of using this tool is that the obtained information can be used in clinical practice to tailor intervention programs for patients with kidney stones.
The findings of this study pointed out that the mean score of perceived severity among female patients was significantly lower than that in male patients. Other determinants did not show significant statistical gender differences. Several studies illustrated that perceived severity was an important factor that predicts behavior [27, 28]. Our findings also indicated that patients with a good daily intake of water (2 liters and more) reported higher perceived severity compared to the poor water intake group (lower than 2 liters). Based on this finding, it seems that educational interventions are needed to improve perceived severity, especially among female patients.
Our findings indicated that only 9% of patients reported two or more liters of water intake during the day. In this regard, Gordon et al., in their study reported that the majority of patients (about 60%) were unsuccessful in fluid intake [24]. Increased fluid intake has been proposed as an inexpensive strategy to prevent kidney stones [29]. The comparison between the findings of the present research and those obtained in similar studies conducted abroad illustrated that the water intake is much lower among Iranian patients with kidney stones compared to those in developing countries. These findings can be a warning to health policymakers in Iran and should be the focus of special attention. These results pointed to the necessity of providing training on the easiest way to prevent relapse among Iranian patients with kidney stones (more than two liters per day).
The present study has some limitations. Firstly, our sample included patients with kidney stones in the west of Iran, and representatives of other populations were not available in the current study. Secondly, according to the non-probability of data collection, our findings maybe not be generalized to other groups of patients with kidney stones. Thirdly, the failure to evaluate the external validity of the questionnaire was another limitation of our study. Future studies are necessary to evaluate the external validity of this questionnaire. Finally, another limitation of the present study was the lack of attention to the threshold of thirst.
Conclusions
Moussa and Chakra, in their study among patients with kidney or ureteral stones in Beirut, reported that most patients were not receiving kidney stone prevention counseling [30]. Urologists and clinical nurses play a critical role in advice for patients' prevention of kidney stones. In addition, designing an evidence-based intervention for patients with kidney stones in order to increase their water intake is important. The current provided significant information for health planning programmers to develop water intake promotion programs among patients with kidney stones. In other words, the use of our scale may be useful for guiding implementers to evaluate the determinants related to water intake and the development of effective health promotion programs among Iranian patients with kidney stones. In general, it was found that using the current questionnaire helps us to identify the predictors of low water intake in patients with kidney stones. A thorough understanding of the problems posed to water intake can be helpful in focusing interventions for patients with kidney stones. Finally, the validity and reliability of the instrument proposed for the cognitive constructs are adequate to support the use of this questionnaire in research on the prediction of water intake among Iranian patients with kidney stones.
Abbreviations
| ICC | Intra-class Correlation Coefficient |
| CIA | Classical Item Analysis |
| CITC | Corrected Item-Total Correlation |
| CVI | Content Validity Index |
| CVR | Content Validity Ratio |
| EFA | Exploratory Factor Analysis |
| KMO | Kaiser–Meyer–Olkin |
| IRH | Imam Reza Hospital |
| SPSS | Statistical Package for Social Sciences |
Compliance with ethical guidelines
The Research Ethics Committee at Deputy of Research of the Kermanshah University of Medical Sciences in the west of Iran approved the study protocol (KUMS.REC.1397.045). Furthermore, the participants were provided with the participant information statement and signed the written consent form. Individual personal information was kept confidential.
Acknowledgments
The authors would like to thank Kermanshah University of Medical Sciences, Kermanshah, Iran. Furthermore, we sincerely thank all patients participating in the study for their cooperation.
Authorsʼ contributions
MMA and FJ contributed to the conception and design of the research; HF, MMA, and FJ contributed to the acquisition design; FJ contributed to the analysis and interpretation of the data. MMA contributed to the scientific edit. All authors approved the final manuscript.
Funding/Support
This study was funded by the Kermanshah University of Medical Sciences, Kermanshah, Iran (research number: 97191). The funding organizations had no role in the design of the study, collection, analysis, and interpretation of data and in writing the manuscript.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
1. López M, Hoppe B. History, epidemiology and regional diversities of urolithiasis. Pediatric Nephrology. 2010; 25(1):49-59. [DOI:10.1007/s00467-008-0960-5] [PMID] [PMCID]
2. Mikawlrawng K, Kumar S, Vandana R. Current scenario of urolithiasis and the use of medicinal plants as antiurolithiatic agents in Manipur (North East India): a review. International Journal of herbal Medicine. 2014; 2(1):1-12.
3. Coe FL, Evan A, Worcester E. Kidney stone disease. The Journal of Clinical Investigation. 2005; 115(10):2598-608. [DOI:10.1172/JCI26662] [PMID] [PMCID]
4. Rule AD, Roger VL, Melton LJ, Bergstralh EJ, Li X, Peyser PA, et al. Kidney stones associate with increased risk for myocardial infarction. Journal of the American Society of Nephrology. 2010; 21(10):1641-4. [DOI:10.1681/ASN.2010030253] [PMID] [PMCID]
5. Chauhan CK, Joshi MJ, Vaidya AD. Growth inhibition of struvite crystals in the presence of herbal extract Commiphora wightii. Journal of Materials Science: Materials in Medicine. 2009; 20(1):85-92. [DOI:10.1007/s10856-008-3489-z] [PMID]
6. Safarinejad MR. Adult urolithiasis in a population-based study in Iran: prevalence, incidence, and associated risk factors. Urological Research. 2007; 35(2):73-82. [DOI:10.1007/s00240-007-0084-6] [PMID]
7. Edvardsson VO, Indridason OS, Haraldsson G, Kjartansson O, Palsson R. Temporal trends in the incidence of kidney stone disease. Kidney International. 2013; 83(1):146-52. [DOI:10.1038/ki.2012.320] [PMID]
8. Dhanalakshmi S, Gayathri R, Vishnupriya V. Correlation between inadequate intake of water and prevalence of Renal Calculi–A survey. Journal of Pharmaceutical Sciences and Research. 2017; 9(4):429.
9. Pearle MS, Goldfarb DS, Assimos DG, Curhan G, Denu-Ciocca CJ, Matlaga BR, et al. Medical management of kidney stones: AUA guideline. The Journal of Urology. 2014; 192(2):316-24. [DOI:10.1016/j.juro.2014.05.006] [PMID]
10. Lotan Y, Buendia Jiménez I, Lenoir‐Wijnkoop I, Daudon M, Molinier L, Tack I, et al. Primary prevention of nephron-lithiasis is cost-effective for a national healthcare system. BJU International. 2012; 110(11):1060-7. [DOI:10.1111/j.1464-410X.2012.11212.x] [PMID]
11. Kok G, Gottlieb NH, Peters GJ, Mullen PD, Parcel GS, Ruiter RA, et al. A taxonomy of behaviour change methods: an Intervention Mapping approach. Health Psychology Review. 2016; 10(3):297-312. [DOI:10.1080/17437199.2015.1077155] [PMID] [PMCD]
12. Borghi L, Schianchi T, Meschi T, Guerra A, Allegri F, Maggiore U, et al. Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria. New England Journal of Medicine. 2002; 346(2):77-84. [DOI:10.1056/NEJMoa010369] [PMID]
13. O'Connor SM, Jardine AG, Millar K. The prediction of self-care behaviors in end-stage renal disease patients using Leventhal's Self-Regulatory Model. Journal of Psychosomatic Research. 2008; 65(2):191-200. [DOI:10.1016/j.jpsychores..02.008] [PMID]
14. Rich A, Brandes K, Mullan B, Hagger MS. Theory of planned behavior and adherence in chronic illness: a meta-analysis. Journal of Behavioral Medicine. 2015; 38(4):673-88. [DOI:10.1007/s10865-015-9644-3] [PMID]
15. McCauley LR, Dyer AJ, Stern K, Hicks T, Nguyen MM. Factors influencing fluid intake behavior among kidney stone formers. The Journal of Urology. 2012; 187(4):1282-6. [DOI:10.1016/j.juro.2011.11.111] [PMID]
16. Khalil A, Abdalrahim M. Knowledge, attitudes, and practices towards prevention and early detection of chronic kidney disease. International Nursing Review. 2014; 61(2):237-45. [DOI:10.1111/inr.12085] [PMID]
17. Lindberg M, Fernandes MA. Self-efficacy in relation to limited fluid intake amongst Portuguese haemodialysis patients. Journal of Renal Care. 2010; 36(3):133-8. [DOI:10.1111/j.1755-6686.2010.00182.x] [PMID]
18. Arya LA, Banks C, Gopal M, Northington GM. Development and testing of a new instrument to measure fluid intake, output, and urinary symptoms: the questionnaire-based voiding diary. American Journal of Obstetrics and Gynecology. 2008; 198(5):1-7. [DOI:10.1016/j.ajog.2008.01.049] [PMID]
19. Lindberg M, Wikström B, Lindberg P. Fluid Intake Appraisal Inventory: development and psychometric evaluation of a situation-specific measure for haemodialysis patients' self-efficacy to low fluid intake. Journal of Psychosomatic Research. 2007; 63(2):167-73. [DOI:10.1016/j.jpsychores.2007.03.013] [PMID]
20. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommend-ations. Research in Nursing & Health. 2007; 30(4):459-67. [DOI:10.1002/nur.20199] [PMID]
21. Lawshe CH. A quantitative approach to content validity. Personnel Psychology. 1975; 28(4):563-75. [DOI:10.1111/j.1744-6570.1975.tb01393.x]
22. Hayton JC, Allen DG, Scarpello V. Factor retention decisions in exploratory factor analysis: A tutorial on parallel analysis. Organizational Research Methods. 2004; 7(2):191-205. [DOI:10.1177/1094428104263675]
23. Crary MA, Mann GD, Groher ME. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Archives of Physical Medicine and Rehabilitation. 2005; 86(8):1516-20. [DOI:10.1016/j.apmr.2004.11.049] [PMID]
24. Gordon EJ, Prohaska TR, Gallant M, Siminoff LA. Self-care strategies and barriers among kidney transplant recipients: a qualitative study. Chronic Illness. 2009; 5(2):75-91. [DOI:10.1177/1742395309103558] [PMID]
25. Tarplin S, Monga M, Stern KL, McCauley LR, Sarkissian C, Nguyen MM. Predictors of reporting success with increased fluid intake among kidney stone patients. Urology. 2016; 88:49-56. [DOI:10.1016/j.urology.2015.10.024] [PMID]
26. Leung SF, Lee KL, Lee SM, Leung SC, Hung WS, Lee WL, et al. Psychometric properties of the SCOFF questionnaire (Chinese version) for screening eating disorders in Hong Kong secondary school students: A cross-sectional study. International Journal of Nursing Studies. 2009; 46(2):239-47. [DOI:10.1016/j.ijnurstu.2008.09.004] [PMID]
27. Ferrer RA, Klein WM, Avishai A, Jones K, Villegas M, Sheeran P. When does risk perception predict protection motivation for health threats? A person-by-situation analysis. PloS One. 2018; 13(3):e0191994. [DOI:10.1371/journal.pone.0191994] [PMID] [PMCID]
28. Nie R, Han Y, Xu J, Huang Q, Mao J. Illness perception, risk perception and health promotion self-care behaviors among Chinese patient with type 2 diabetes: A cross-sectional survey. Applied Nursing Research. 2018; 39:89-96. [DOI:10.1016/j.apnr.2017.11.010] [PMID]
29. Cheungpasitporn W, Rossetti S, Friend K, Erickson SB, Lieske JC. Treatment effect, adherence, and safety of high fluid intake for the prevention of incident and recurrent kidney stones: a systematic review and meta-analysis. Journal of Nephrology. 2016; 29(2):211-9. [DOI:10.1007/s40620-015-0210-4] [PMID] [PMCID]
30. Moussa M, Abou Chakra M. Patient's perception of kidney stone prevention within the emergency department and its adherence factors: a single institution study. BMC Emergency Medicine. 2019; 19(1):1-7. [DOI:10.1186/s12873-019-0263-0] [PMID] [PMCID]
Article Type: Research Article |
Subject:
Health Education and Promotion
Received: 2023/01/21 | Accepted: 2023/05/14 | Published: 2023/06/20
Received: 2023/01/21 | Accepted: 2023/05/14 | Published: 2023/06/20
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Hamadan University of Medical Sciences.
Published by UMSHA Press
Journal Tel: +989025126654
Publisher Tel: +985136014377
Website: http://ajnpp.umsha.ac.ir
Email: avicennajnpp[at]gmail.com
