

Volume 7, Issue 2 (May 2020)
Avicenna J Neuro Psycho Physiology 2020, 7(2): 69-76 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Salim Bahrami S H, Jahan F, Asadzadeh Dehraei H, Sotoodeh Asl N. Effectiveness of Mindfulness Training on Anxiety Reduction as well as Improvement of Life Quality and Perceived Academic Control of Students. Avicenna J Neuro Psycho Physiology 2020; 7 (2) :69-76
URL: http://ajnpp.umsha.ac.ir/article-1-313-en.html
URL: http://ajnpp.umsha.ac.ir/article-1-313-en.html


1- Ph.D. Candidate of Educational Psychology, Semnan Branch, Islamic Azad University, Semnan, Iran
2- Assistant Professor, Department of Psychology, Semnan Branch, Islamic Azad University, Semnan, Iran
3- Associate Professor, Department of Psychology, Semnan Branch, Islamic Azad University, Semnan, Iran
4- Associate Professor, Department of Psychology, Semnan Branch, Islamic Azad University, Semnan, Iran ,Sotodeh1@yahoo.com
2- Assistant Professor, Department of Psychology, Semnan Branch, Islamic Azad University, Semnan, Iran
3- Associate Professor, Department of Psychology, Semnan Branch, Islamic Azad University, Semnan, Iran
4- Associate Professor, Department of Psychology, Semnan Branch, Islamic Azad University, Semnan, Iran ,
Full-Text [PDF 1572 kb]
(1351 Downloads)
| Abstract (HTML) (4208 Views)
Table 2. Mean±SD results of the research variables
Full-Text: (1544 Views)
Background
In recent years, mindfulness in the scientific community has received a great deal of attention and is defined as moment-by-moment awareness of the experience gained from targeted attention along with the uncritical acceptance of existing experiences [1]. Most studies have focused on evaluating the effectiveness of mindfulness-based interventions. Accordingly, mindfulness training interventions have recently been associated with a variety of health outcomes, such as pain reduction [2], anxiety, and depression [3], as well as reduced rumination [4].
Mindfulness is a therapeutic process that focuses on purposeful and non-judgmental attention along with accepting experiences, confessing to them, living in the moment, reducing consciousness and distressing behaviors significantly [5], and encouraging the person to reduce conflict with thoughts and feelings. The person becomes aware of the automatic functions of the mind and daily activities when practicing mindfulness exercises and provides the necessary context for moment-by-moment awareness of thoughts, feelings, and control [6]. Mindfulness in two-way interactions can improve mental and physical health [7] and establish an artistic interaction among physical, cognitive, and emotional processes [8].
Depression, anxiety, and stresses of modern life cause severe injuries to the human body and psyche and increase physical illnesses, anxiety, and depression [9]. One of the concerns of the educational system is the issue of student anxiety, which is difficult for many students to endure [10]. Anxiety is a familiar word for educated people and is one of the most essential motivational and cognitive variables that significantly affect academic achievement, learning, performance, as well as attention, focus, and retrieval of learner's information [11]. The existence of anxiety at a moderate level is considered a conciliatory response [12]; however, severe anxiety is the cause of many physical illnesses, mental illnesses, behavioral disturbances, and adverse reactions. Such responses may manifest as decreased attention and concentration, increased forgetfulness and distraction, increased error rate, decreased creative capacity, unpredictable response speed, reduced organizational power, as well as short and long-term memory impairment [13]. As anxiety increases, many aspects of psychological indicators decline, one of which is the quality of life [14].
Some researchers believe that the quality of life is the amount of enjoyment that individuals receive from their lives. The most important opportunity and potential for enjoying are a happy and healthy physical and psychological life [15]. Another important psychological factor in students’ mental health that protects them from stress and depression is perceived academic control. Perceived academic control is one of the variables consistent with optimism that enhances student’s cognitive performance and commitment to obtaining a degree [16]. Perceived academic control refers to the use of a set of methods and tools aimed at reading thought, controlling, and mastering academic behavior. Since it is linked to human beliefs, it plays a role in people's cognitive appraisal of events [17]. Perceived academic control is consciously assessed as learners' beliefs of their ability (high or low) to influence academic outcomes [18]. Studies aimed at examining perceived academic control in the classroom have shown that learners with high academic control (those with an internal control source) have a high degree of control over their academic performances and are more eager to learn, compared to those with a low perceived academic control (those with external control resources) [19].
The results of a study performed by Aránega, Sánchez, and Pérez [20] showed that mindfulness training in Spanish students was effective in lowering their stress levels. In another study, Riet, Levett-Jones, and Aquino-Russell found that mindfulness meditation had a positive effect on stress, anxiety, depression, burnout, wellbeing, and empathy in nursing students. Findings from Kinser et al. [21] showed that mindfulness training significantly reduced perceived stress, anxiety, and specific aspects of burnout in health care professionals and trainees after the intervention. In the studies conducted by Greeson, Toohey, and Pearce [22], they reported that mindfulness awareness workshops had a significant effect on students' stress reduction, subjectivity, and self-care (i.e., exercise, sleep, and social support).
A review of past studies has shown that mindfulness plays an essential role in people's lives. However, in the mentioned studies, mindfulness has been examined with other variables, such as death anxiety, positive and negative emotions, mental health, marital satisfaction, academic self-concept, depression, and assertiveness. However, researchers, in particular, have not examined the effectiveness of mindfulness training on reducing anxiety, improving quality of life, and perceived academic control of students. Many students have good cognitive abilities; however, since they are not capable of thinking constructively in different situations, they have poor academic performance and low quality of life. Anxiety also harms the efficiency and flourishing of their talents, which can limit the potential of educational opportunities for them. The present study can help identify the variables that influence student life and improve the educational process. Therefore, given the high prevalence of these psychological symptoms and the effects of these symptoms on students' performance and health, the main question of the present study was whether mindfulness training has an impact on reducing anxiety as well as improving the quality of life and perceived academic control of students?
Objectives
The present study aimed to determine the effectiveness of mindfulness training on reducing anxiety and improving the quality of life as well as perceived academic control of students.
Materials and Methods
This quasi-experimental study was conducted based on a pretest-posttest design with a control group. The study population consisted of all undergraduate students of Sari Branch, Islamic Azad University, Sari, Iran, in the academic year 2018-19. Initially, undergraduate students were identified and screened using the Beck anxiety scale, World Health Organization quality of life questionnaire, and perceived academic control scale by Perry et al. Subsequently, those who obtained the cut-off scores above 16 in anxiety, lower than 70 in quality of life, and lower than 20 in academic control were selected as participants.
A total of 40 individuals were randomly divided into two groups of case (n=20) and control (n=20) based on the inclusion criteria and results of the pretest. The inclusion criteria were: 1) age range between 19 and 23 years, 2) undergraduate students in the academic year of 2018-19, 3) no use of psychiatric drugs, and 4) no use of educational program before and during mindfulness intervention. On the other hand, the students with a history of psychotic disorders, mania, hypomania, personality disorders, cognitive impairments, such as dementia, substance abuse, hearing or speech problems, and those who received psychotherapies during the month before the study and were absent for more than two sessions were excluded from the study.
Beck Anxiety Questionnaire
It is a 21-item self-report questionnaire aimed to measure the severity of anxiety in adolescents and adults. The subjects were asked to choose one of four options indicating the severity of anxiety. The items are scored based on a 4-point Likert scale from 0-3. Each of the test items describes one of the most common symptoms of anxiety (i.e., mental, physical, and phobic symptoms). Therefore, the total score of this questionnaire is ranged from 0 to 63. The score ranges of 0-7, 8-15, 16-25, and 26-63 indicate no or the least, mild, moderate, and severe level of anxiety, respectively [23]. Beck [24] estimated the internal consistency of this tool (Cronbach's alpha) at 0.92. Moreover, the validity of this questionnaire was obtained at 0.75 using the test-retest method with the correlation coefficient from 0.30 to 0.76. In the present study, the reliability of this questionnaire was determined at 0.87 using Cronbach's alpha.
World Health Organization Quality of Life Questionnaire
This self-report tool was designed by the World Health Organization to assess people's quality of life. This 26-item questionnaire is a short version of the World Health Organization Quality of Life Questionnaire. The first two questions assess the quality of life and overall health of the individual, and the other 24 questions examine the four main domains, including physical health, mental health, social relationships, and environmental health. The participants were asked to answer each question on a 5-point Likert scale. This test was standardized in Iran by Nedjat et al. [25] and Cronbach's alpha coefficients of the physical health, mental health, social relationships, and environmental health were obtained at 0.87, 0.74, 0.55, and 0.74, respectively. These coefficients indicated the optimal reliability of the test. In the present study, the reliability of the questionnaire was estimated to be 0.92 using Cronbach's Alpha Coefficient.
Perceived academic control Questionnaire
This 8-item questionnaire consists of two subscales, namely academic responsibility and controllability with positive (n=4) and negative (n=4) sentences that are scored from strongly agree (1) to disagree (5) [26]. In a study conducted by Perry et al. [27], the reliability of this scale was obtained at 0.80 using Cronbach's Alpha. The Iranian version of this scale was validated by Esfandiari et.al [28] with the validity and reliability of 0.77 and 0.82, respectively. In the present study, the reliability of the questionnaire was obtained at 0.91 using Cronbach's Alpha.
The experimental group was subjected to eight 2-h mindfulness training sessions for two months. On the other hand, the control group received no pieces of training. The contents of the training sessions were selected based on the Browns and Marlatt Mindfulness protocol. Table 1 tabulates the stages of the training sessions as follows:
After the end of the sessions, posttest sessions were administered for both groups. The data were analyzed in SPSS software (version 25) using covariance analysis.
Results
According to the results of the Skewness and Kurtosis tests, the research variables were normally distributed. The Skewness and Kurtosis of all the variables were obtained at the range of ±2. Moreover, the results of the Kolmogorov-Smirnov test indicated that the assumption of a normal distribution of variables could not be rejected (P˃0.05). The level of significance for all three variables (i.e., anxiety, quality of life, and perceived academic control) was more than 0.05 indicating the normal distribution of variables. Furthermore, Leven's test results showed that the significance level for all variables was greater than 0.05 (P<0.05), which indicated that the distribution of dependent variables at the group level (confounding variable) was homogeneous and similar.
According to Table 3, the results of univariate analysis of covariance (ANCOVA) showed that mindfulness intervention influenced all three main variables, namely anxiety, quality of life, and perceived academic control (P<0.05). The level of significance for all three main variables was less than the presumed value of 0.05, which indicated that mindfulness caused a significant decrease in anxiety and a significant increase in the quality of life and perceived academic control. Similarly, a comparison of the mean of the control and case groups showed that the rates of anxiety reduction were 0.14 and 2.24 in the control and case groups, respectively. Furthermore, the level of increase in the quality of life of the control and case groups were determined at 0.32 and 8.33, respectively. In addition, the rates of increased perceived academic control were estimated at 0.22 in the control and 4.38 in the case groups. The effect size indicated the extent of the impact of the intervention on the dependent variables. Comparison of the effect sizes showed that mindfulness had the greatest effect on
Mindfulness is a therapeutic process that focuses on purposeful and non-judgmental attention along with accepting experiences, confessing to them, living in the moment, reducing consciousness and distressing behaviors significantly [5], and encouraging the person to reduce conflict with thoughts and feelings. The person becomes aware of the automatic functions of the mind and daily activities when practicing mindfulness exercises and provides the necessary context for moment-by-moment awareness of thoughts, feelings, and control [6]. Mindfulness in two-way interactions can improve mental and physical health [7] and establish an artistic interaction among physical, cognitive, and emotional processes [8].
Depression, anxiety, and stresses of modern life cause severe injuries to the human body and psyche and increase physical illnesses, anxiety, and depression [9]. One of the concerns of the educational system is the issue of student anxiety, which is difficult for many students to endure [10]. Anxiety is a familiar word for educated people and is one of the most essential motivational and cognitive variables that significantly affect academic achievement, learning, performance, as well as attention, focus, and retrieval of learner's information [11]. The existence of anxiety at a moderate level is considered a conciliatory response [12]; however, severe anxiety is the cause of many physical illnesses, mental illnesses, behavioral disturbances, and adverse reactions. Such responses may manifest as decreased attention and concentration, increased forgetfulness and distraction, increased error rate, decreased creative capacity, unpredictable response speed, reduced organizational power, as well as short and long-term memory impairment [13]. As anxiety increases, many aspects of psychological indicators decline, one of which is the quality of life [14].
Some researchers believe that the quality of life is the amount of enjoyment that individuals receive from their lives. The most important opportunity and potential for enjoying are a happy and healthy physical and psychological life [15]. Another important psychological factor in students’ mental health that protects them from stress and depression is perceived academic control. Perceived academic control is one of the variables consistent with optimism that enhances student’s cognitive performance and commitment to obtaining a degree [16]. Perceived academic control refers to the use of a set of methods and tools aimed at reading thought, controlling, and mastering academic behavior. Since it is linked to human beliefs, it plays a role in people's cognitive appraisal of events [17]. Perceived academic control is consciously assessed as learners' beliefs of their ability (high or low) to influence academic outcomes [18]. Studies aimed at examining perceived academic control in the classroom have shown that learners with high academic control (those with an internal control source) have a high degree of control over their academic performances and are more eager to learn, compared to those with a low perceived academic control (those with external control resources) [19].
The results of a study performed by Aránega, Sánchez, and Pérez [20] showed that mindfulness training in Spanish students was effective in lowering their stress levels. In another study, Riet, Levett-Jones, and Aquino-Russell found that mindfulness meditation had a positive effect on stress, anxiety, depression, burnout, wellbeing, and empathy in nursing students. Findings from Kinser et al. [21] showed that mindfulness training significantly reduced perceived stress, anxiety, and specific aspects of burnout in health care professionals and trainees after the intervention. In the studies conducted by Greeson, Toohey, and Pearce [22], they reported that mindfulness awareness workshops had a significant effect on students' stress reduction, subjectivity, and self-care (i.e., exercise, sleep, and social support).
A review of past studies has shown that mindfulness plays an essential role in people's lives. However, in the mentioned studies, mindfulness has been examined with other variables, such as death anxiety, positive and negative emotions, mental health, marital satisfaction, academic self-concept, depression, and assertiveness. However, researchers, in particular, have not examined the effectiveness of mindfulness training on reducing anxiety, improving quality of life, and perceived academic control of students. Many students have good cognitive abilities; however, since they are not capable of thinking constructively in different situations, they have poor academic performance and low quality of life. Anxiety also harms the efficiency and flourishing of their talents, which can limit the potential of educational opportunities for them. The present study can help identify the variables that influence student life and improve the educational process. Therefore, given the high prevalence of these psychological symptoms and the effects of these symptoms on students' performance and health, the main question of the present study was whether mindfulness training has an impact on reducing anxiety as well as improving the quality of life and perceived academic control of students?
Objectives
The present study aimed to determine the effectiveness of mindfulness training on reducing anxiety and improving the quality of life as well as perceived academic control of students.
Materials and Methods
This quasi-experimental study was conducted based on a pretest-posttest design with a control group. The study population consisted of all undergraduate students of Sari Branch, Islamic Azad University, Sari, Iran, in the academic year 2018-19. Initially, undergraduate students were identified and screened using the Beck anxiety scale, World Health Organization quality of life questionnaire, and perceived academic control scale by Perry et al. Subsequently, those who obtained the cut-off scores above 16 in anxiety, lower than 70 in quality of life, and lower than 20 in academic control were selected as participants.
A total of 40 individuals were randomly divided into two groups of case (n=20) and control (n=20) based on the inclusion criteria and results of the pretest. The inclusion criteria were: 1) age range between 19 and 23 years, 2) undergraduate students in the academic year of 2018-19, 3) no use of psychiatric drugs, and 4) no use of educational program before and during mindfulness intervention. On the other hand, the students with a history of psychotic disorders, mania, hypomania, personality disorders, cognitive impairments, such as dementia, substance abuse, hearing or speech problems, and those who received psychotherapies during the month before the study and were absent for more than two sessions were excluded from the study.
Beck Anxiety Questionnaire
It is a 21-item self-report questionnaire aimed to measure the severity of anxiety in adolescents and adults. The subjects were asked to choose one of four options indicating the severity of anxiety. The items are scored based on a 4-point Likert scale from 0-3. Each of the test items describes one of the most common symptoms of anxiety (i.e., mental, physical, and phobic symptoms). Therefore, the total score of this questionnaire is ranged from 0 to 63. The score ranges of 0-7, 8-15, 16-25, and 26-63 indicate no or the least, mild, moderate, and severe level of anxiety, respectively [23]. Beck [24] estimated the internal consistency of this tool (Cronbach's alpha) at 0.92. Moreover, the validity of this questionnaire was obtained at 0.75 using the test-retest method with the correlation coefficient from 0.30 to 0.76. In the present study, the reliability of this questionnaire was determined at 0.87 using Cronbach's alpha.
World Health Organization Quality of Life Questionnaire
This self-report tool was designed by the World Health Organization to assess people's quality of life. This 26-item questionnaire is a short version of the World Health Organization Quality of Life Questionnaire. The first two questions assess the quality of life and overall health of the individual, and the other 24 questions examine the four main domains, including physical health, mental health, social relationships, and environmental health. The participants were asked to answer each question on a 5-point Likert scale. This test was standardized in Iran by Nedjat et al. [25] and Cronbach's alpha coefficients of the physical health, mental health, social relationships, and environmental health were obtained at 0.87, 0.74, 0.55, and 0.74, respectively. These coefficients indicated the optimal reliability of the test. In the present study, the reliability of the questionnaire was estimated to be 0.92 using Cronbach's Alpha Coefficient.
Perceived academic control Questionnaire
This 8-item questionnaire consists of two subscales, namely academic responsibility and controllability with positive (n=4) and negative (n=4) sentences that are scored from strongly agree (1) to disagree (5) [26]. In a study conducted by Perry et al. [27], the reliability of this scale was obtained at 0.80 using Cronbach's Alpha. The Iranian version of this scale was validated by Esfandiari et.al [28] with the validity and reliability of 0.77 and 0.82, respectively. In the present study, the reliability of the questionnaire was obtained at 0.91 using Cronbach's Alpha.
The experimental group was subjected to eight 2-h mindfulness training sessions for two months. On the other hand, the control group received no pieces of training. The contents of the training sessions were selected based on the Browns and Marlatt Mindfulness protocol. Table 1 tabulates the stages of the training sessions as follows:
After the end of the sessions, posttest sessions were administered for both groups. The data were analyzed in SPSS software (version 25) using covariance analysis.
Results
According to the results of the Skewness and Kurtosis tests, the research variables were normally distributed. The Skewness and Kurtosis of all the variables were obtained at the range of ±2. Moreover, the results of the Kolmogorov-Smirnov test indicated that the assumption of a normal distribution of variables could not be rejected (P˃0.05). The level of significance for all three variables (i.e., anxiety, quality of life, and perceived academic control) was more than 0.05 indicating the normal distribution of variables. Furthermore, Leven's test results showed that the significance level for all variables was greater than 0.05 (P<0.05), which indicated that the distribution of dependent variables at the group level (confounding variable) was homogeneous and similar.
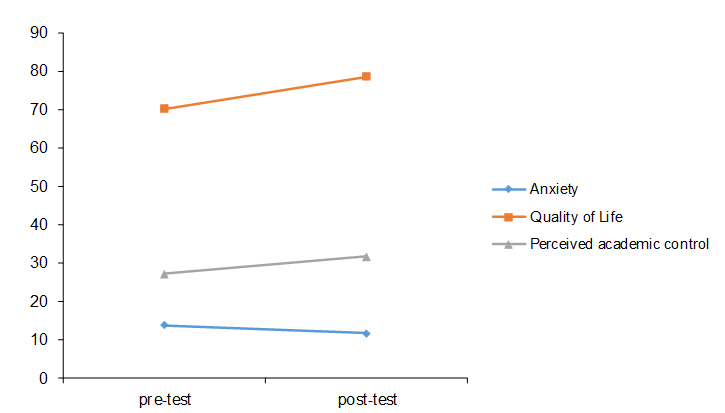
According to Table 3, the results of univariate analysis of covariance (ANCOVA) showed that mindfulness intervention influenced all three main variables, namely anxiety, quality of life, and perceived academic control (P<0.05). The level of significance for all three main variables was less than the presumed value of 0.05, which indicated that mindfulness caused a significant decrease in anxiety and a significant increase in the quality of life and perceived academic control. Similarly, a comparison of the mean of the control and case groups showed that the rates of anxiety reduction were 0.14 and 2.24 in the control and case groups, respectively. Furthermore, the level of increase in the quality of life of the control and case groups were determined at 0.32 and 8.33, respectively. In addition, the rates of increased perceived academic control were estimated at 0.22 in the control and 4.38 in the case groups. The effect size indicated the extent of the impact of the intervention on the dependent variables. Comparison of the effect sizes showed that mindfulness had the greatest effect on
| Sessions | Content |
| 1 |
|
| 2 |
|
| 3 |
|
| 4 |
|
| 5 |
|
| 6 |
|
| 7 |
|
| 8 |
|
Table 2. Mean±SD results of the research variables
| Variables | Levels | Statistics | Control group | Case group |
| Anxiety | Pretest | Mean | 14.09 | 13.81 |
| SD | 3.17 | 3.95 | ||
| Posttest | Mean | 13.95 | 11.57 | |
| SD | 3.21 | 2.79 | ||
| Quality of Life | Pretest | Mean | 65.15 | 70.26 |
| SD | 8.26 | 8.47 | ||
| Posttest | Mean | 65.47 | 78.59 | |
| SD | 8.01 | 9.72 | ||
| Perceived academic control | Pretest | Mean | 28.19 | 27.21 |
| SD | 1.28 | 4.21 | ||
| Posttest | Mean | 28.41 | 31.59 | |
| SD | 4.37 | 5.08 |
Table 3. Results of univariate analysis of covariance to examine the impact of the intervention on the main variables
| Dependent variable | Source change | Sum of squares | df | F | P-value | Effect size |
| Anxiety | Group (mindfulness) | 45.40 | 1 | 37.44 | ˂0.001 | 0.503 |
| Quality of Life | Group (mindfulness) | 730.13 | 1 | 260.15 | ˂0.001 | 0.875 |
| Perceived academic control | Group (mindfulness) | 156.66 | 1 | 154.43 | ˂0.001 | 0.807 |
Figure 1. Comparison of research variables in pre-test and post-test
the quality of life with an effect size of 0.875 and then on perceived academic control with a coefficient of 0.807.
Discussion
The present study aimed to determine the effectiveness of mindfulness training on anxiety reduction and improvement of life quality as well as perceived academic control of students. The results showed that mindfulness training had a positive and significant effect on reducing students’ anxiety. This finding was consistent with the results of the studies conducted by Aránega, Sánchez and Pérez [20], Kinser et al. [21], as well as Petterson and Olson [30]. In general, the hypothesis can be stated that based on cognitive perspective, anxiety, and anxiety disorders are the results of unrealistic and irrational false beliefs, especially exaggerated irrational beliefs about natural hazards. The cognitive perspective holds that people acquire and interpret information and use it to solve life’s problems.
Rational-emotional therapy (a clinical approach based on Schacht's theory) pursues two goals. The first aim causes people to question these fundamental but mistaken beliefs, and the second one seeks to make more constructive beliefs in place of them. "Meditation" is one of the techniques in mindfulness, which is an activity of mental awareness, including emotions, memories, and dreams. We can recognize our mistakes and adjust our minds to think and respond more realistically and honestly through meditation. Moreover, we learn to have less unrealistic expectations of people and things around us, and therefore, we experience less frustration which leads to the improvement of relationships; accordingly, life becomes more stable and satisfying. We create and develop a broad sense of what is going on around us. One of the mechanisms of mindfulness is "metacognitive awareness," which refers to the beliefs that individuals have about their thinking. This knowledge includes beliefs about specific types of thinking, as well as beliefs about memory efficiency or focus power. These beliefs influence how individuals respond and how their thoughts are regulated.
In mindfulness exercises, students gain the ability to break through the vicious cycle of negative self-thoughts by fully focusing on what is happening now and here. Overall, the results of the current study indicated that mindfulness techniques are an effective and preventive strategy in reducing anxiety. Moreover, providing students with these skills enables them to reduce their anxiety in anxious situations while reducing the incidence, prevalence, and complications. It is worth mentioning that mindfulness has an undeniable effect on reducing students’ anxiety.
The results of this study showed the positive and significant effect of mindfulness training on the improvement of quality of life among students. This finding was consistent with the results of the studies performed by Raj et al. [31]. In general, the hypothesis can be said that mindfulness is an all-round awareness that helps broad and open minds and embraces emotions and physical phenomena as they happen. As a result, mindfulness training in students controls thoughts and emotions and improves their quality of life and positive emotions.
The power of emotion regulation and self-management in the individual is increased with mindfulness training, and people directly adjust their emotions and change the level of their positive quality of life. Mindfulness training sessions empower the person to face stressful situations because of its hidden mechanism, such as observing without judgment, increasing awareness, being present at the moment, as well as accepting and avoiding avoidance, such as student life.
Mindfulness skills are predictors of self-regulatory behavior and positive emotional states that increase individual satisfaction and improve quality of life. An increase in the awareness of a person's own beliefs, thought processes, and thoughts through learning mindfulness skills lead the person to evaluate different situations better and earlier, take appropriate action, and become less likely to have difficulty in making decisions.
In the same line, mindfulness is a therapeutic process that refers to purposeful and non-judgmental attention along with accepting experiences, confessing to it, living in the moment that reduces the level of consciousness and distressing behaviors significantly, and encouraging one to reduce conflict with thoughts and feelings. One becomes aware of the automatic functions of the mind and daily activities by practicing mindfulness exercises. This provides the necessary context for the moment-by-moment awareness of thoughts and feelings that help him/her to control them.
Mindfulness can improve both mental and physical health. Therefore, in order to plan to improve the level of health and quality of life in students, which in turn improves the educational environment, they should be aware of their health status and attitude towards their health and quality of life. The results of this study showed that mindfulness training had an impact on improving the quality of life. Since life has many dimensions, including physical, mental, social, and spiritual, mindfulness exercises are designed to affect all of these aspects. As such, it should improve the quality of life. It seems that such training can improve the quality of life of students. The constant exercise of mindfulness increases awareness, cognition, as well as awareness of the body, emotions, and thoughts. Since teaching mindfulness skills to students enable them to self-regulate, think, and act in the face of stressful situations and situations, it leads to creating a happier and healthier life by reducing stress and focusing on abilities and talents.
The results showed that mindfulness training had a positive and significant effect on students’ perceived academic control. This finding was in line with the results of a study carried out by McManus et al. [32]. Students experience greater well-being and health; moreover, they learn more behavioral skills when attending mindfulness training sessions, which can then deepen awareness and increase emotion management, reduce stress, and enhance homework pursuits as well as perceived academic control.
Following that, the power of self-management and students' perceived academic control increases with an increase in mindfulness. Individuals who experience an increase in the state of mindfulness are focused on the present and change internal and external stimuli. As a result, they become aware of the symptoms of academic control, and this awareness prevents them from postponing academic matters for any reason [33]. Mindfulness means paying attention to the present in a specific and purposeful way without judgment. Meditation and mindfulness exercises lead to increased self-awareness and acceptance in individuals [34]. As a result, the person who is more aware of his/her thoughts, feelings, and emotions is less affected by negative and destructive thoughts as well as unpleasant emotions. Therefore, mindfulness education leads the students to be more informed and scientific in their performance and academic achievement.
Although this study paves the way for the effectiveness of mindfulness training, it suffers from notable limitations. In this study, the control group consisted of students with no group meetings. Therefore, active mechanisms related to the group experience, such as group acceptance, as well as to the educator, such as empathy or other items in the training may not be included in the results. Moreover, cautions should be considered in generalizing the results of the study to other groups of vulnerable students due to a high level of anxiety and life quality of the students and poor perceived academic control. Based on the results of this study, it is hoped that by controlling other confounding factors such as age, gender, as well as social and cultural status, the study limitations be reduced, and the stage can be set for the generalization of the results. Given the effectiveness of mindfulness education in students, it is possible to provide workshops for students and their families to empower them, thereby preventing or reducing problems and consequences.
Conclusions
According to the findings of this study, it is recommended that mindfulness training be provided to develop and promote students' psychological health.
Compliance with ethical guidelines
All ethical principles were considered in this study. The participants were informed about the research objectives and procedures. Moreover, written informed consent was obtained from them. They were also assured about the confidentiality of their information, and they were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them. This study was extracted from a Ph.D. thesis in counseling submitted to the Semnan Branch, Islamic Azad University, Semnan, Iran. The study protocol was also approved by the Ethics Committee of the Semnan Branch, Islamic Azad University, Semnan, Iran (IR.IAU.SEMNAN.REC.1397.011).
Funding/Support
This study received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declare that they have no conflict of interests.
References
Discussion
The present study aimed to determine the effectiveness of mindfulness training on anxiety reduction and improvement of life quality as well as perceived academic control of students. The results showed that mindfulness training had a positive and significant effect on reducing students’ anxiety. This finding was consistent with the results of the studies conducted by Aránega, Sánchez and Pérez [20], Kinser et al. [21], as well as Petterson and Olson [30]. In general, the hypothesis can be stated that based on cognitive perspective, anxiety, and anxiety disorders are the results of unrealistic and irrational false beliefs, especially exaggerated irrational beliefs about natural hazards. The cognitive perspective holds that people acquire and interpret information and use it to solve life’s problems.
Rational-emotional therapy (a clinical approach based on Schacht's theory) pursues two goals. The first aim causes people to question these fundamental but mistaken beliefs, and the second one seeks to make more constructive beliefs in place of them. "Meditation" is one of the techniques in mindfulness, which is an activity of mental awareness, including emotions, memories, and dreams. We can recognize our mistakes and adjust our minds to think and respond more realistically and honestly through meditation. Moreover, we learn to have less unrealistic expectations of people and things around us, and therefore, we experience less frustration which leads to the improvement of relationships; accordingly, life becomes more stable and satisfying. We create and develop a broad sense of what is going on around us. One of the mechanisms of mindfulness is "metacognitive awareness," which refers to the beliefs that individuals have about their thinking. This knowledge includes beliefs about specific types of thinking, as well as beliefs about memory efficiency or focus power. These beliefs influence how individuals respond and how their thoughts are regulated.
In mindfulness exercises, students gain the ability to break through the vicious cycle of negative self-thoughts by fully focusing on what is happening now and here. Overall, the results of the current study indicated that mindfulness techniques are an effective and preventive strategy in reducing anxiety. Moreover, providing students with these skills enables them to reduce their anxiety in anxious situations while reducing the incidence, prevalence, and complications. It is worth mentioning that mindfulness has an undeniable effect on reducing students’ anxiety.
The results of this study showed the positive and significant effect of mindfulness training on the improvement of quality of life among students. This finding was consistent with the results of the studies performed by Raj et al. [31]. In general, the hypothesis can be said that mindfulness is an all-round awareness that helps broad and open minds and embraces emotions and physical phenomena as they happen. As a result, mindfulness training in students controls thoughts and emotions and improves their quality of life and positive emotions.
The power of emotion regulation and self-management in the individual is increased with mindfulness training, and people directly adjust their emotions and change the level of their positive quality of life. Mindfulness training sessions empower the person to face stressful situations because of its hidden mechanism, such as observing without judgment, increasing awareness, being present at the moment, as well as accepting and avoiding avoidance, such as student life.
Mindfulness skills are predictors of self-regulatory behavior and positive emotional states that increase individual satisfaction and improve quality of life. An increase in the awareness of a person's own beliefs, thought processes, and thoughts through learning mindfulness skills lead the person to evaluate different situations better and earlier, take appropriate action, and become less likely to have difficulty in making decisions.
In the same line, mindfulness is a therapeutic process that refers to purposeful and non-judgmental attention along with accepting experiences, confessing to it, living in the moment that reduces the level of consciousness and distressing behaviors significantly, and encouraging one to reduce conflict with thoughts and feelings. One becomes aware of the automatic functions of the mind and daily activities by practicing mindfulness exercises. This provides the necessary context for the moment-by-moment awareness of thoughts and feelings that help him/her to control them.
Mindfulness can improve both mental and physical health. Therefore, in order to plan to improve the level of health and quality of life in students, which in turn improves the educational environment, they should be aware of their health status and attitude towards their health and quality of life. The results of this study showed that mindfulness training had an impact on improving the quality of life. Since life has many dimensions, including physical, mental, social, and spiritual, mindfulness exercises are designed to affect all of these aspects. As such, it should improve the quality of life. It seems that such training can improve the quality of life of students. The constant exercise of mindfulness increases awareness, cognition, as well as awareness of the body, emotions, and thoughts. Since teaching mindfulness skills to students enable them to self-regulate, think, and act in the face of stressful situations and situations, it leads to creating a happier and healthier life by reducing stress and focusing on abilities and talents.
The results showed that mindfulness training had a positive and significant effect on students’ perceived academic control. This finding was in line with the results of a study carried out by McManus et al. [32]. Students experience greater well-being and health; moreover, they learn more behavioral skills when attending mindfulness training sessions, which can then deepen awareness and increase emotion management, reduce stress, and enhance homework pursuits as well as perceived academic control.
Following that, the power of self-management and students' perceived academic control increases with an increase in mindfulness. Individuals who experience an increase in the state of mindfulness are focused on the present and change internal and external stimuli. As a result, they become aware of the symptoms of academic control, and this awareness prevents them from postponing academic matters for any reason [33]. Mindfulness means paying attention to the present in a specific and purposeful way without judgment. Meditation and mindfulness exercises lead to increased self-awareness and acceptance in individuals [34]. As a result, the person who is more aware of his/her thoughts, feelings, and emotions is less affected by negative and destructive thoughts as well as unpleasant emotions. Therefore, mindfulness education leads the students to be more informed and scientific in their performance and academic achievement.
Although this study paves the way for the effectiveness of mindfulness training, it suffers from notable limitations. In this study, the control group consisted of students with no group meetings. Therefore, active mechanisms related to the group experience, such as group acceptance, as well as to the educator, such as empathy or other items in the training may not be included in the results. Moreover, cautions should be considered in generalizing the results of the study to other groups of vulnerable students due to a high level of anxiety and life quality of the students and poor perceived academic control. Based on the results of this study, it is hoped that by controlling other confounding factors such as age, gender, as well as social and cultural status, the study limitations be reduced, and the stage can be set for the generalization of the results. Given the effectiveness of mindfulness education in students, it is possible to provide workshops for students and their families to empower them, thereby preventing or reducing problems and consequences.
Conclusions
According to the findings of this study, it is recommended that mindfulness training be provided to develop and promote students' psychological health.
Compliance with ethical guidelines
All ethical principles were considered in this study. The participants were informed about the research objectives and procedures. Moreover, written informed consent was obtained from them. They were also assured about the confidentiality of their information, and they were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them. This study was extracted from a Ph.D. thesis in counseling submitted to the Semnan Branch, Islamic Azad University, Semnan, Iran. The study protocol was also approved by the Ethics Committee of the Semnan Branch, Islamic Azad University, Semnan, Iran (IR.IAU.SEMNAN.REC.1397.011).
Funding/Support
This study received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declare that they have no conflict of interests.
References
- Baer RA, Krietemeyer J. Overview of mindfulness-and acceptance-based treatment approaches. Mindfulness-based treatment approaches: clinician's guide to evidence base and applications. New York: Elsevier; 2006. P. 1-27.
- Bakosh LS, Mortlock JM, Querstret D, Morison L. Audio-guided mindfulness training in schools and its effect on academic attainment: contributing to theory and practice. Learning and Instruction. 2018; 58:34-41. [DOI:10.1016/j.
learninstruc.2018.04.012] - Bradley RT, McCraty R, Atkinson M, Tomasino D, Daugherty A, Arguelles L. Emotion self-regulation, psychophysiological coherence, and test anxiety: results from an experiment using electrophysiological measures. Applied Psychophysiology and Biofeedback. 2010; 35(4):261-83. [DOI:10.1007/s10484-010-9134-x] [PMID]
- Bishop SR. What do we really know about mindfulness-based stress reduction? Psychosomatic Medicine. 2002; 64(1):71-83. [DOI:10.1097/00006842-200201000-00010] [PMID]
- Bellizzi KM, Smith AW, Reeve BB, Alfano CM, Bernstein L, Meeske K, et al. Posttraumatic growth and health-related quality of life in a racially diverse cohort of breast cancer survivors. Journal of Health Psychology. 2010; 15(4):615-26. [DOI:10.1177/1359105309356364] [PMID]
- Edelman M, Ficorelli C. A measure of success: nursing students and test anxiety. Journal for Nurses in Professional Development. 2005; 21(2):55-9. [DOI:10.1097/00124645-200503000-00004] [PMID]
- Duprey EB, McKee LG, O'Neal CW, Algoe SB. Stressful life events and internalizing symptoms in emerging adults: The roles of mindfulness and gratitude. Mental Health & Prevention. 2018; 12:1-9. [DOI:10.1016/j.mhp.2018.08.003]
- Evans S, Ferrando S, Findler M, Stowell C, Smart C, Haglin D. Mindfulness-based cognitive therapy for generalized anxiety disorder. Journal of Anxiety Disorders. 2008; 22(4):716-21. [DOI:10.1016/j.janxdis.2007.07.005] [PMID]
- Andela CD, Lobatto DJ, Pereira AM, van Furth WR, Biermasz NR. How non-functioning pituitary adenomas can affect health-related quality of life: a conceptual model
and literature review. Pituitary. 2018; 21(2):208-16. [DOI:10.1007/s11102-017-0860-4] [PMID] [PMCID] - Fleury-Bahi G, Pol E, Navarro O. Handbook of environmental psychology and quality of life research. Cham, Switzerland: Springer International Publishing; 2017.
- Grossman P, Tiefenthaler-Gilmer U, Raysz A, Kesper U. Mindfulness training as an intervention for fibromyalgia: evidence of postintervention and 3-year follow-up benefits in well-being. Psychotherapy and Psychosomatics. 2007; 76(4):226-33. [DOI:10.1159/000101501] [PMID]
- Schunk DH. Academic achievement. The Corsini Encyclopedia of Psychology. 2010; 6:1-2. [DOI:10.1002/
9780470479216.corpsy0006] - Sreeramareddy CT, Shankar PR, Binu VS, Mukhopadhyay C, Ray B, Menezes RG. Psychological morbidity, sources of stress and coping strategies among undergraduate medical students of Nepal. BMC Medical Education. 2007; 7(1):26. [DOI:10.1186/1472-6920-7-26] [PMID] [PMCID]
- Stephens RL. Imagery: a treatment for nursing student anxiety. Journal of Nursing Education. 1992; 31(7):314-20. [PMID]
- Kabat‐Zinn J. Mindfulness‐based interventions in context: past, present, and future. Clinical Psychology: Science and Practice. 2003; 10(2):144-56. [DOI:10.1093/clipsy.bpg016]
- Lavender R, Nguyen-Rodriguez ST, Spruijt-Metz D. Teaching the whole student: Perceived academic control in college art instruction. Studies in Art Education. 2010; 51(3):198-218. [DOI:10.1080/00393541.2010.11518803]
- Michalak J, Burg J, Heidenreich T. Don't forget your body: mindfulness, embodiment, and the treatment of depression. Mindfulness. 2012; 3(3):190-9. [DOI:10.1007/s12671-012-0107-4]
- Patel NK, Nivethitha L, Mooventhan A. Effect of a yoga based meditation technique on emotional regulation, self-compassion and mindfulness in college students. Explore. 2018; 14(6):443-7. [DOI:10.1016/j.explore.2018.06.008] [PMID]
- Ruthig JC, Hanson BL, Marino JM. A three-phase examination of academic comparative optimism and perceived academic control. Learning and Individual Differences. 2009; 19(4):435-9. [DOI:10.1016/j.lindif.
2009.03.004] - Aránega AY, Sánchez RC, Pérez CG. Mindfulness' effects on undergraduates' perception of self-knowledge and stress levels. Journal of Business Research. 2019; 101:441-6. [DOI:10.1016/j.jbusres.2019.01.026]
- Kinser P, Braun S, Deeb G, Carrico C, Dow A. “Awareness is the first step”: an interprofessional course on mindfulness & mindful-movement for healthcare professionals and students. Complementary Therapies in Clinical Practice. 2016; 25:18-25. [DOI:10.1016/j.ctcp.2016.08.003] [PMID]
- Greeson JM, Toohey MJ, Pearce MJ. An adapted, four-week mind–body skills group for medical students: reducing stress, increasing mindfulness, and enhancing self-care. Explore. 2015; 11(3):186-92. [DOI:10.1016/j.explore.
2015.02.003] [PMID] - Phan T, Carter O, Adams C, Waterer G, Chung LP, Hawkins M, et al. Discriminant validity of the hospital anxiety and depression scale, beck depression inventory (II) and beck anxiety inventory to confirmed clinical diagnosis of depression and anxiety in patients with chronic obstructive pulmonary disease. Chronic Respiratory Disease. 2016; 13(3):220-8. [DOI:10.1177/1479972316634604] [PMID] [PMCID]
- van der Riet P, Levett-Jones T, Aquino-Russell C. The effectiveness of mindfulness meditation for nurses and nursing students: an integrated literature review. Nurse Education Today. 2018; 65:201-11. [DOI:10.1016/j.nedt.
2018.03.018] [PMID] - Nedjat S, Naieni KH, Mohammad K, Majdzadeh R, Montazeri A. Quality of life among an Iranian general population sample using the World Health Organization’s quality of life instrument (WHOQOL-BREF). International Journal of Public Health. 2011; 56(1):55-61. [DOI:10.1007/
s00038-010-0174-z] [PMID] - Perry RP. Perceived (academic) control and causal thinking in achievement settings. Canadian Psychology/Psychologie Canadienne. 2003; 44(4):312-31. [DOI:10.1037/h0086956]
- Perry RP, Hladkyj S, Pekrun RH, Pelletier ST. Academic control and action control in the achievement of college students: a longitudinal field study. Journal of Educational Psychology. 2001; 93(4):776-89.
- Esfandiari S, Omidvar N, Eini-Zinab H, Doustmohammadian A, Amirhamidi Z. Associations among food insecurity, academic performance, and weight status in primary schoolchildren in Tehran, Iran: a cross-sectional study. Journal of Nutrition Education and Behavior. 2018; 50(2):109-17. [DOI:10.1016/j.jneb.2017.05.365] [PMID]
- Bowen S, Chawla N, Marlatt GA. Mindfulness-based relapse prevention for addictive behaviors: a clinician's guide. New York: Guilford Press; 2011.
- Petterson H, Olson BL. Effects of mindfulness-based interventions in high school and college athletes for reducing stress and injury, and improving quality of life. Journal of Sport Rehabilitation. 2017; 26(6):578-87. [DOI:10.1123/jsr.2016-0047] [PMID]
- Raj S, Sachdeva SA, Jha R, Sharad S, Singh T, Arya YK, et al. Effectiveness of mindfulness based cognitive behavior therapy on life satisfaction, and life orientation of adolescents with depression and suicidal ideation. Asian Journal of Psychiatry. 2019; 39:58-62. [DOI:10.1016/
j.ajp.2018.12.001] [PMID] - McManus F, Surawy C, Muse K, Vazquez-Montes M, Williams JM. A randomized clinical trial of mindfulness-based cognitive therapy versus unrestricted services for health anxiety (hypochondriasis). Journal of Consulting and Clinical Psychology. 2012; 80(5):817-28. [DOI:10.1037/
a0028782] [PMID] [PMCID] - Paul NA, Stanton SJ, Greeson JM, Smoski MJ, Wang L. Psychological and neural mechanisms of trait mindfulness in reducing depression vulnerability. Social Cognitive and Affective Neuroscience. 2012; 8(1):56-64. [DOI:10.1093/
scan/nss070] [PMID] [PMCID] - Ruthig JC, Haynes TL, Stupnisky RH, Perry RP. Perceived academic control: mediating the effects of optimism and social support on college students’ psychological health. Social Psychology of Education. 2009; 12(2):233-49. [DOI:10.1007/s11218-008-9079-6]
Article Type: Research Article |
Subject:
Clinical Psychology
Received: 2020/08/13 | Accepted: 2020/05/10 | Published: 2020/05/10
Received: 2020/08/13 | Accepted: 2020/05/10 | Published: 2020/05/10
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Hamadan University of Medical Sciences.
Published by UMSHA Press
Journal Tel: +989025126654
Publisher Tel: +985136014377
Website: http://ajnpp.umsha.ac.ir
Email: avicennajnpp[at]gmail.com
