




BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://ajnpp.umsha.ac.ir/article-1-198-en.html



2- Department of Clinical Psychology, Faculty of Psychology and Social Sciences, Islamic Azad University, Roodehen Branch, Iran. ,
Introduction
A Healthy society can be formed by families or couples with a good and healthy relationship. Kindness and love are one of the foundations of this kind of healthy relationship [1]. When a spouse does not value the relationship as much as the other one does or when the essential needs of a spouse are ignored, marital satisfaction or intimacy will be diminished and also or the reason for living together will be disappeared. Intimacy is a process, in which individuals try to approach each other and discover their similarities and differences in emotions, thoughts, and behaviors [2]. Satisfactory relationships between couples can be measured through mutual interest, the amount of caregiving, and mutual acceptance and understanding [3]. Therefore, it is essential to examine the mental health of couples to help them improve their marital relationship. According to the World Health Organization (WHO), mental health is not limited to the absence of mental disorders but is a state of well-being and comfort that enables an individual to realize his abilities and talents [4]. Also, he can adapt to the natural pressures of daily life and influence his community with useful and beneficial activities.
Mental health issues and problems, especially mental illnesses, have distinct and transparent economic and social consequences for societies. If couples feel comfortable about mutual life, it provides them with welfare, security, and health, enhances their appreciation of their abilities, and improves parental responsibility [5]. Marital satisfaction is associated with a high level of mental health, and the higher the marital satisfaction, the more likely a person is to experience positive emotions [6]. People who are more satisfied with their lives use more effective and suitable coping styles, experience deeper positive emotions and feelings and have higher general health. Marital dissatisfaction is associated with poorer health, depressive symptoms, personality problems, inappropriate behaviors, and poor social status [7].
On the other hand, psychological well-being has been extensively studied through the last two decades, and its goal has expanded from individual life to social interaction [8]. Mental well-being involves the individual’s perceptions of the degree, in which goals are aligned and delineated with the functional outcomes. They are achieved by continuous evaluations that lead to internal and relatively lasting satisfaction in life. Well-being refers to a sense of health that includes a full awareness of the entirety and integrity of all aspects of the individual. Mental well-being encompasses individuals’ cognitive values of their lives, and people differently rate their conditions depending on their expectations, values, and past experiences [9]. Mental well-being is a psychological component of quality of life that is defined as individuals’ perceptions of their own lives in the domain of emotional behaviors, mental functioning, and mental health dimensions and has two components. The first component includes cognitive judgment about how individuals are progressing in their lives. The second component encompasses the level of pleasant experiences. Some researchers have conceptualized psychological well-being in terms of specific components or processes, such as emotional processes [10].
Intimacy is also a real and fundamental need in humans. Individuals differ according to individual differences based on their severity and type of intimacy. Intimacy is a dynamic process based on mutual trust and respect. It is a real need with an intrinsic root and stems from a fundamental need for fondness [11]. On the other hand, in unsuccessful and dissolved marriages, lack of intimacy unwittingly ends the couples’ relationships. For example, in an authentic study on causes of divorce in the United States, 80% of divorced men and women reported a lack of intimacy developed gradually, as well as a lack of feeling of love and valuation as the causes of their separation and failure in marriage [12].
On the one hand, resilient individuals who do not have self-destructive behaviors are emotionally calm and capable of coping with unpleasant and distasteful conditions [13]. Those with high resilience are more likely to show positive emotions when confronted with emotional events of a neutral and obscure nature; which may be due to their ability to successfully cope with difficult situations. This is especially true for interpersonal situations. On the other hand, hope is a factor closely associated with psychological well-being and resilience. It is a motivational factor and also an optimistic state of mind. Hope energizes and equips humans, and acts as an accelerator for work and activity [14]. The purpose of this study was to predict psychological well-being based on marital intimacy, resilience, and mental health of couples in Tehran.
Materials and Methods
This descriptive-correlational study was conducted on 150 couples referring to the counseling centers in districts 1 and 2 of Tehran between Feb and May 2019 selected by the convenience sampling. First, 3-6 counseling centers were identified in districts 1 and 2 of Tehran, and then the questionnaires were distributed among those willing to participate in the study. Inclusion criteria were referral to the counseling centers, the age range of 20-45 years, and the exclusion criterion was providing incomplete information. Before administering the questionnaires, the subjects were informed about the research objectives and they were also assured of the confidentiality of the information and using them only for the research purposes.
Ryff Psychological Well-Being Scale
Ryff developed a self-report tool in 1989 to test his theoretical model of psychological well-being, which is one of the essential measures of psychological well-being. The first version of this tool had 120 questions. In subsequent years, its shorter versions including 40, 84, 42, 24, 18, 14, 9, and 3 questions were compiled based on research on its psychometric properties. Ryff believed that the 84-item version of the test is more capable of determining psychological well-being than other versions. He edited the 84-question version in 1989. In the 84-item version, 14 questions are assigned to each component, including self-acceptance, mastery of the environment, positive relationships with others, personal growth, purpose in life, and self-compliance. The total score of these six components is an overall psychological well-being score [15].
In Iran, its reliability was obtained through retest with the coefficient of 0.82 for the overall score, 0.71 for self-acceptance, 0.77 for positive relationships with others, 0.78 for self-compliance, 0.77 for environmental mastery, 0.70 for having a purpose in life and 0.78 for personal growth. Life satisfaction tests, the Oxford Happiness Questionnaire, and the Rosenberg Self-esteem Questionnaire were also used to assess the validity of the questionnaire. Correlation scores of these tests with psychological well-being were 0.47, 0.58, and 0.46, respectively [16]. In the present study, the validity and reliability of the questionnaire were 0.77 and 0.79, respectively.
Connor-Davidson Resilience Scale (CD-RISC)
This 25-item questionnaire was developed by Conner and Davidson in 2003 to measure resilience in different individuals by a review of studies conducted on resilience in 1979–1991. It is scored on a Likert scale ranging from 0 to 100. The higher scores indicate greater resilience of the respondent and vice versa. The cut-off point for this questionnaire is 50. In other words, a score above 50 indicates resilience, and the scores over 50 represent the greater resilience, and vice versa [17]. In Iran, the reliability of the questionnaire was estimated at 0.84 using the Cronbach’s alpha coefficient. In the present study, the validity and reliability of the questionnaire were 0.75 and 0.70, respectively.
General Health Questionnaire (GHQ-28)
This questionnaire was developed by Goldberg in 1972 for identifying people with minor psychiatric disorders from those who consider themselves healthy. The original version of the GHQ consists of 60 questions; however, several shorter versions have also been developed. The GHQ-28 is applicable for everyone in the community and has four sub-scales of physical symptoms, anxiety and insomnia, dysfunctional social functioning, and depression. It takes about 10-12 min to answer the questions [18]. The reliability of the scale using the retest method for the whole questionnaire was 0.72, and for the subscales of physical symptoms, anxiety, and insomnia, social dysfunction, and depression were 0.60, 0.68, 0.57, and 0.58, respectively. Also, regarding its reliability, the alpha coefficient obtained by the two-way split-half method for the whole questionnaire was 0.93, and for the subscales of physical symptoms, anxiety, and insomnia, social dysfunction, and depression were 0.86, 0.84, 0.68 and 0.77, respectively. Also, the internal consistency using Cronbach’s alpha for the whole questionnaire was 0.90, and for the subscales of physical symptoms, anxiety, and insomnia, social dysfunction, and depression were 0.76, 0.84, 0.61, and 0.88, respectively [19]. In the present study, the validity and reliability of the scale were 0.75 and 0.88, respectively.
Marital Intimacy Scale
This scale, developed by Thompson and Walker in 1983, has 17 questions and was designed to measure the amount of couples’ intimacy. The range of scores on each question varies from 1 (never) to 7 (always) and higher scores indicate greater intimacy. This scale has a good internal consistency with the alpha coefficient of 0.91 to 0.97 [20]. Each participant’s score is obtained by summing the scores of the questions and dividing them by 17. The reliability coefficient of the whole scale using Cronbach’s alpha method was 0.96, which indicates its acceptable reliability [21]. Also, the validity and reliability of the questionnaire in this research were 0.79 and 0.86, respectively.
Data were analyzed using descriptive and inferential statistics (Pearson correlation coefficient and multiple linear regression). Descriptive statistics were used to calculate frequencies, determine central indices, and depict charts and graphs. The significant level was 0.05. Also, all statistical calculations were performed using SPSS V. 22 software.
Results
Of 300 participants, 75 (25%) were in the age group of 20-25 years, 69 (23%) in the age group of 26-30 years, 103 cases (34.3%) in the age group of 31-35 years, and 53 (17.7%) were in the age group of 36-40 years.
According to Table 1, there was a positive correlation between mean psychological well-being (188.4±21.3) and total marital intimacy (65.1±11.9; r=0.47) and resiliency (63.7±11.8; r=0.35), whereas there was a negative relationship between the components of psychological well-being and the components and total score of mental health (P<0.01).

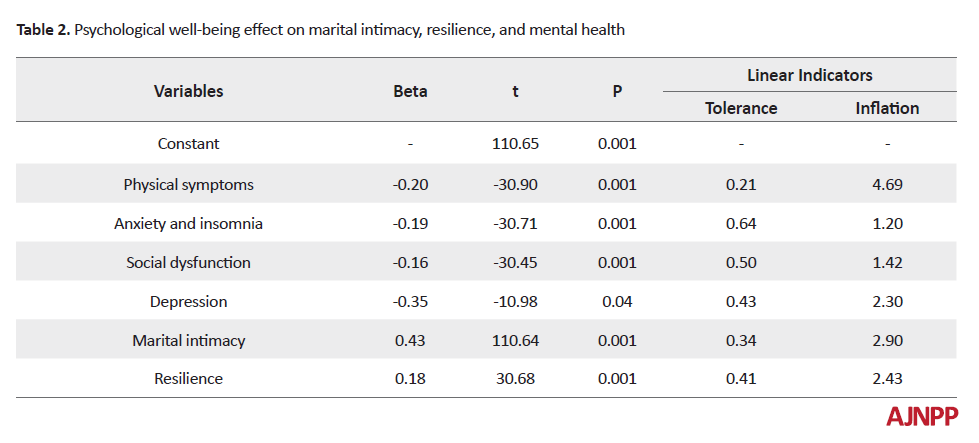
The results of the regression model also showed that marital intimacy (B=0.43) and resiliency (B=0.18) could positively affect psychological well-being, and also mental health (B=-0.39) negatively predicted psychological well-being.
Psychological well-being as the criterion variable, and marital intimacy, resilience, and mental health as predictor variables were entered into the regression equation. The results of this model showed that the subscales of marital intimacy, resilience, and mental health were able to predict psychological well-being (F=54.58, P<.0001). Therefore, there were multiple relationships between marital intimacy, resiliency, and mental health and psychological well-being.
Discussion
The results showed that there was a positive correlation between psychological well-being and marital intimacy (r=0.47, P<0.0001), whereas there was a negative correlation between psychological well-being and the components of mental health (P<0.0001). Also, the results of the regression model showed that marital intimacy, resilience, and mental health were able to predict psychological well-being (P<0.0001) (Table 2).
It can be argued that young couples satisfied with their marital life have a positive interpersonal relationship; they are highly unified and support each other in various aspects of the marriage, and understand each other in many family and leisure time activities. They can manage conflicts constructively, interact with their families mutually and positively, and understand different aspects of life, such as financial issues. As a result, couples who consider their spouses as compassionate and accessible sources of support have a feeling of security and self-esteem and are characterized by higher levels of health and well-being [22]. Also, marital intimacy, especially in the beginning of the marriage, provides a framework for couples to experience love, intimacy, pleasure, and affection in the best possible way. Research has shown that marital intimacy increases intimacy between couples, improves marital satisfaction, and consequently, increases their mental health [23]. The present study showed that there is a positive and significant relationship between marital satisfaction and marital intimacy, and mental health in the age group of 31-40 years, and marital satisfaction could predict 38% of the variance of mental health positively and significantly, which is in line with the results of other studies [24].
In general, our findings indicated the importance of marital satisfaction and sexual satisfaction as two essential dimensions of marital quality of life and marriage stability in enhancing the psychological health of married people in different age groups. Marital satisfaction and intimacy are not limited to a specific period in the marriage life cycle. Psychological well-being is greater in cases who have experienced marital and sexual satisfaction in their parents. Couples who are over 40 years of age may also experience greater mental health if they have marital and sexual satisfaction. Marital intimacy is a relational process, in which the couples enjoy each other in marriage and being at home. Some psychologists believe that marital satisfaction is a coincidence between the present status of couples and the expected one. Accordingly, marital satisfaction is proven when the present statue is compatible with the considered expectation of a person. The couple’s perception and comprehension of the extent, severity, and range of the problems in their relationships can affect their marital satisfaction. Marital satisfaction is also a consequence of marital agreement that is internally perceived. It is a personal experience in the marriage that is only assessed by an individual in response to the enjoyment of the marital relationship, which can be affected by many factors [25].
In this study, the questionnaire was used for data collection. Therefore, orientation could have been generated in the collected information, as some participants may answer some questions incorrectly to represent themselves with a more favorable state. One of the limitations of the present study was using the available sampling method, which limits the generalizability of the findings. Another limitation of the present study was its correlation methodology that limits the causal inference about the resulting relationships. The limited research population to couples referring to the counseling centers in districts 1 and 2 of Tehran can affect the generalization of results to other cities. Researchers can also use other methods, such as interviews to obtain accurate information. It is suggested that the present study be conducted as an empirical study to investigate the effects of different training methods on resiliency, marital intimacy, and general health of couples. It is also recommended that similar studies be carried out in other cities so that the results of the present study are comparable to their results. Based on the provided information, it is necessary to emphasize the necessity of reviewing the educational strategies of couples to improve the resiliency, marital intimacy, and general health of couples.
Conclusion
It can be concluded that by improving the components of psychological well-being, marital intimacy and resilience increase, whereas by increasing the level of psychological well-being, mental health can be increased.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages and signed the informed consent; they were also assured about the confidentiality of their information. Moreover, they were allowed to leave the study whenever they wish, and if desired. Also, they were explained that the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally in preparing all parts of the research.
Conflict of interest
The authors declared no conflict of interest.
References
1.Amiri-Majd, M, Hosseini, SF, Jafari A. [Comparing the quality of life and marital intimacy among parents of children with Down syndrome, parents of children with learning disabilities, and parents of normal children (Persian)]. Journal of Learning Disabilities. 2014; 4(1):38-55.
2.Atkins L, Brown RG, Leigh PN, Goldstein LH. Marital relationships in amyotrophic lateral sclerosis. Amyotrophic Lateral Sclerosis. 2010; 11(4):344-50. [DOI:10.3109/17482960903307797] [PMID]
3.Balderrama-Durbin C, Snyder DK, Cigrang J, Talcott GW, Tatum J, Baker M, et al. Combat disclosure in intimate relationships: Mediating the impact of partner support on posttraumatic stress. Journal of Family Psychology. 2013; 27(4):560-8. [DOI:10.1037/a0033412] [PMID]
4.Bloch L, Haase CM, Levenson RW. Emotion regulation predicts marital satisfaction: More than a wives’ tale. Emotion. 2014; 14(1):130-44. [DOI:10.1037/a0034272] [PMID] [PMCID]
5.Boehm JK, Kubzansky LD. The heart’s content: The association between positive psychological well-being and cardiovascular health. Psychological Bulletin. 2012; 138(4):655-91. [DOI:10.1037/a0027448] [PMID]
6.Bögels SM, Hellemans J, van Deursen S, Römer M, van der Meulen R. Mindful parenting in mental health care: Effects on parental and child psychopathology, parental stress, parenting, coparenting, and marital functioning. Mindfulness. 2014; 5(5):536-51. [DOI:10.1007/s12671-013-0209-7]
7.Bränström R, Kvillemo P, Brandberg Y, Moskowitz JT. Self-report mindfulness as a mediator of psychological well-being in a stress reduction intervention for cancer patients-A randomized study. Annals of Behavioral Medicine. 2010; 39(2):151-61. [DOI:10.1007/s12160-010-9168-6] [PMID]
8.Cabral I, Grilo A, Cruz-Machado V. A decision-making model for lean, agile, resilient and green supply chain management. International Journal of Production Research. 2012; 50(17):4830-45. [DOI:10.1080/00207543.2012.657970]
9.Canavarro MC, Silva S, Moreira H. Is the link between posttraumatic growth and anxious symptoms mediated by marital intimacy in breast cancer patients? European Journal of Oncology Nursing. 2015; 19(6):673-9. [DOI:10.1016/j.ejon.2015.04.007] [PMID]
10.Cash M, Whittingham K. What facets of mindfulness contribute to psychological well-being and depressive, anxious, and stress-related symptomatology? Mindfulness. 2010; 1(3):177-82. [DOI:10.1007/s12671-010-0023-4]
11.Choi YU, Baek YM. The effects of family of origin health, marital intimacy, conflict between daughter-in-law and mother-in-law on marital satisfaction in married woman. The Korean Journal of Rehabilitation Psychology. 2010; 17(17):145-64.
12.Clare L, Nelis SM, Whitaker CJ, Martyr A, Markova IS, Roth I, et al. Marital relationship quality in early-stage dementia: Perspectives from people with dementia and their spouses. Alzheimer Disease & Associated Disorders. 2012; 26(2):148-58. [DOI:10.1097/WAD.0b013e318221ba23] [PMID]
13.Connor KM, Davidson JR. Development of a new resilience scale: The Connor‐Davidson resilience scale (CD‐RISC). Depression and anxiety. 2003; 18(2):76-82. [DOI:10.1002/da.10113] [PMID]
14.Desouza KC, Flanery TH. Designing, planning, and managing resilient cities: A conceptual framework. Cities. 2013; 35:89-99. [DOI:10.1016/j.cities.2013.06.003]
15.Ryff CD. Psychological well-being revisited: Advances in the science and practice of eudaimonia. Psychotherapy and Psychosomatics. 2014; 83(1):10-28. [DOI:10.1159/000353263] [PMID] [PMCID]
16.Diener E, Tay L, Myers DG. The religion paradox: If religion makes people happy, why are so many dropping out?. Journal of Personality and Social Psychology. 2011; 101(6):1278-90. [DOI:10.1037/a0024402] [PMID]
17.Engle JM, McElwain NL. Parental depressive symptoms and marital intimacy at 4.5 years: Joint contributions to mother-child and father-child interaction at 6.5 years. Developmental Psychology. 2013; 49(12):2225-35. [DOI:10.1037/a0032450] [PMID]
18.Finkbeiner NM, Epstein NB, Falconier MK. Low intimacy as a mediator between depression and clinic couple relationship satisfaction. Personal Relationships. 2013; 20(3):406-21. [DOI:10.1111/j.1475-6811.2012.01415.x]
19.Greenwood J, Guner N, Kocharkov G, Santos C. Technology and the changing family: A unified model of marriage, divorce, educational attainment, and married female labor-force participation. American Economic Journal: Macroeconomics. 2016; 8(1):1-41. [DOI:10.1257/mac.20130156]
20.Habib MF, Tornatore M, De Leenheer M, Dikbiyik F, Mukherjee B. Design of disaster-resilient optical datacenter networks. Journal of Lightwave Technology. 2012; 30(16):2563-73. [DOI:10.1109/JLT.2012.2201696]
21.Haghi F, Allahverdipour H, Nadrian H, Sarbakhsh P, Hashemiparast M, Mirghafourvand M. Sexual problems, marital intimacy and quality of sex life among married women: A study from an Islamic country. Sexual and Relationship Therapy. 2018; 33(3):339-52.
22.Han HR, Lee JM. Mediating effects of work-family balance on the relationship of role recognition in the family, marital intimacy and job satisfaction of married women: Using latent growth curve modeling and autoregressive cross-lagged modeling. Family and Environment Research. 2017; 55(3):263-74. [DOI:10.6115/fer.2017.020]
23.Hatami M, Fadayi M. Effectiveness of schema therapy in intimacy, marital conflict and early maladaptive schemas of women suing for divorce. International Journal of Advanced Biological and Biomedical Research. 2015; 3(3):285-90.
24.Hosseinian S, Yazdi M, Tabatabaee M. Investigating relation between marital communication skills on marital intimacy in married women. Educative-cultural Journal of Family and Women. 2011; 6(18):45-70.
25.Jun EY, Kim S, Chang SB, Oh K, Kang HS, Kang SS. The effect of a sexual life reframing program on marital intimacy, body image, and sexual function among breast cancer survivors. Cancer Nursing. 2011; 34(2):142-9. [DOI:10.1097/NCC.0b013e3181f1ab7a] [PMID]
Received: 2019/04/23 | Accepted: 2019/08/25 | Published: 2019/11/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Hamadan University of Medical Sciences.
Published by UMSHA Press
Journal Tel: +989025126654
Publisher Tel: +985136014377
Website: http://ajnpp.umsha.ac.ir
Email: avicennajnpp[at]gmail.com
