

Volume 5, Issue 3 (August 2018)
Avicenna J Neuro Psycho Physiology 2018, 5(3): 139-146 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Enayati M, Dousti Y, Mirzaian B. The Effectiveness of Acceptance and Commitment Therapy on the Quality of Life and Psychosocial Flexibility of Female Junior High School Students With Special Learning Disorders in Sari. Avicenna J Neuro Psycho Physiology 2018; 5 (3) :139-146
URL: http://ajnpp.umsha.ac.ir/article-1-143-en.html
URL: http://ajnpp.umsha.ac.ir/article-1-143-en.html


1- Department of Psychology, Islamic Azad University, Sari Branch, Sari, Iran.
2- Department of Psychology, Islamic Azad University, Sari Branch, Sari, Iran. ,dousti@iausari.ac.ir
2- Department of Psychology, Islamic Azad University, Sari Branch, Sari, Iran. ,
Full-Text [PDF 705 kb]
(1608 Downloads)
| Abstract (HTML) (4734 Views)


Full-Text: (1373 Views)
Introduction
A learning disorder is a general term that describes disorders in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, whose characteristics cause problems in academic achievement or everyday functioning [1]. The learning disorder in the United States is a term used to describe children, who are impaired in the development of language and communication skills. Children, whose learning problems are primarily because of visual, hearing, movement impairment and or emotional problems, cultural constraints, or general mental retardation, are not a part of this group [2]. Students with learning abnormalities, such as reading, writing, and mathematics show inadequacies in basic reading, writing, and mathematics skills from the very beginning of the school. Reading disorder is marked by special damages in the development of reading skills and math disorders are marked by specific injuries in the acquisition of math skills [3].
The main characteristic of disorder in spelling is that the child’s spelling of the letter is considerably less than the expected level regarding intelligence capacity and educational level [4]. The majority of learners with learning disabilities are regarded as passive learners according to their psychological and behavioral characteristics. They cannot use learning strategies to solve their educational problems and they do not believe in their abilities because the repeated experiences of failure make them disappointed and inefficient. The result of this cycle is the formation of a negative perception of one’s own abilities and a reduction in self-esteem and motivation that paves the way for the emergence of different problems [5].
Various studies have pointed out to the general characteristics of students with learning disabilities; such disabilities include creating problems in the social, emotional, and educational realms [6], failure in the processing of social information [7], limited intimate friends [8], low level of positive social behaviors [9], social problems and low quality of life [10], poor reasoning ability and low problem-solving [11], self-regulation problems of sensory processing [12], and low level of psychological well-being. The full understanding of the above-mentioned disabilities requires attention to the social, emotional, and behavioral areas of individual life [13].
Quality of life is one of the variables that are likely to be weak or impaired because of learning disabilities in students. It seems that the difference in the quality of life of students is because of the ability and the sense of self-efficacy. The quality of life is a range of human needs that are associated with a person’s and group’s perceptions of a sense of well-being [14].
According to the World Health Organization, the quality of life is the perception of individuals regarding the status of life in the realm of culture and the value system, in which they live, which is associated with goals, expectations, criteria, and important affairs [15]. Based on a general agreement among researchers, the quality of life consists of objective factors (mental functions put more emphasis on life satisfaction, while objective factors focus on material needs and participation in interpersonal activities and relationships). Several factors such as age, culture, sex, education, class status, illness, social environment and, in general, behavioral factors, occupation, and resources of adjustment affect an individual’s quality of life [16]. The degree of individuals’ flexibility is among the factors affecting the quality of life.
Flexibility is defined as the ability of cognitive sets to be adapted according to changing environmental stimuli [17]. Cognitive flexibility means the extent, to which a person is open to experience regarding internal and external experiences. This personality trait determines the reaction of individuals against new experiences [18]. Flexibility requires the ability [19]. Flexible people are curious and their lives are rich in terms of experience. Not only they do not avoid encountering internal and external experiences but also they seek new experiences [20].
Among the effective treatments, interventions to improve the quality of life and increase the amount of psychological flexibility is the Acceptance and Commitment Therapy (ACT). The ACT is a cognitive-behavioral therapy based on functional contextualism. It is rooted in a new theory about language and cognition, which is called the theory of mental relations framework. In the ACT, it is assumed that humans consider many of their own internal feelings, emotions, or thoughts annoying and constantly try to change or discharge these inner experiences. These attempts to control them have been ineffective and contradictorily have resulted in the exacerbation of feelings, emotions, and thoughts that the individual initially tried to avoid [21].
The ACT has 6 central processes that lead to psychological flexibility; the processes include acceptance vs. avoidance, dissonance vs. cognitive blending, self as a context vs. conceptualized self, the relation of the present vs. the overcoming of the past and the conceptualized future, emphasis on values vs. the lack of clarity of values and their relation to them, and the commitment vs. being isolated [22]. In fact, this type of treatment is the main purpose of creating psychological flexibility; that is, the ability to make practical choices among different options that are more appropriate, rather than an action merely to avoid disturbing thoughts, emotions, memories or desires, or actually imposed on an individual [23].
The necessity of the present research is to identify and recognize the psychological problems in students with a learning disorder and taking action regarding their treatment and their problems, which should be considered by families and educators. On the one hand, in spite of the expansion of the present research scope, a few studies have been conducted. As long as there is no comprehensive research on effective methods and techniques for improving the quality of life and psychological flexibility, parents, teachers, and education officials cannot plan properly in this regard. Therefore, in order to prevent further problems, paying attention to these students and doing timely and preventive interventions is necessary. The aim of this study was to determine the efficacy of ACT on the quality of life and psychological flexibility of female junior high school students with learning disorders in Sari, Iran.
2. Materials and Methods
The present quasi-experimental study used a Pre-test-Post-test design with a control group. The statistical population included all female junior high school students with special learning disorders in Sari, who were referred to the learning disorders and counseling centers during the academic year 2018-2019. At first, between the two areas of the city, one district was randomly selected and, then, 60 individuals were selected by the convenience sampling method; next, they were randomly assigned to the experimental and the control groups (30 in the experimental group and 30 in the control group). Based on the effect size of 0.25, alpha of 0.5, and power of 0.85 in the two groups, the minimum number of samples to achieve the desired power, 30 individuals in each group and a total of 60 individuals, was determined. The inclusion criteria include the occurrence of a particular learning disorder (reading and math), female gender, junior high school student, and the absence of other serious psychiatric disorders such as schizophrenia and bipolar disorder. The exclusion criteria included the absences of more than 2 sessions, disabling physical illness, and the provision of incomplete information. Both groups completed the 36-item Short Form health survey (SF-36) and the Cognitive Flexibility Inventory (CFI) of Dennis and Vander Wal before the intervention. The experimental group was, then, subjected to the influence of the independent variable for 8 sessions (120 minutes for each session) and the control group received no training. In order to evaluate the effect of the training, the tests for both groups were completely optional. Before starting and participating in the project, they became familiar with the layout specifications.
A learning disorder is a general term that describes disorders in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, whose characteristics cause problems in academic achievement or everyday functioning [1]. The learning disorder in the United States is a term used to describe children, who are impaired in the development of language and communication skills. Children, whose learning problems are primarily because of visual, hearing, movement impairment and or emotional problems, cultural constraints, or general mental retardation, are not a part of this group [2]. Students with learning abnormalities, such as reading, writing, and mathematics show inadequacies in basic reading, writing, and mathematics skills from the very beginning of the school. Reading disorder is marked by special damages in the development of reading skills and math disorders are marked by specific injuries in the acquisition of math skills [3].
The main characteristic of disorder in spelling is that the child’s spelling of the letter is considerably less than the expected level regarding intelligence capacity and educational level [4]. The majority of learners with learning disabilities are regarded as passive learners according to their psychological and behavioral characteristics. They cannot use learning strategies to solve their educational problems and they do not believe in their abilities because the repeated experiences of failure make them disappointed and inefficient. The result of this cycle is the formation of a negative perception of one’s own abilities and a reduction in self-esteem and motivation that paves the way for the emergence of different problems [5].
Various studies have pointed out to the general characteristics of students with learning disabilities; such disabilities include creating problems in the social, emotional, and educational realms [6], failure in the processing of social information [7], limited intimate friends [8], low level of positive social behaviors [9], social problems and low quality of life [10], poor reasoning ability and low problem-solving [11], self-regulation problems of sensory processing [12], and low level of psychological well-being. The full understanding of the above-mentioned disabilities requires attention to the social, emotional, and behavioral areas of individual life [13].
Quality of life is one of the variables that are likely to be weak or impaired because of learning disabilities in students. It seems that the difference in the quality of life of students is because of the ability and the sense of self-efficacy. The quality of life is a range of human needs that are associated with a person’s and group’s perceptions of a sense of well-being [14].
According to the World Health Organization, the quality of life is the perception of individuals regarding the status of life in the realm of culture and the value system, in which they live, which is associated with goals, expectations, criteria, and important affairs [15]. Based on a general agreement among researchers, the quality of life consists of objective factors (mental functions put more emphasis on life satisfaction, while objective factors focus on material needs and participation in interpersonal activities and relationships). Several factors such as age, culture, sex, education, class status, illness, social environment and, in general, behavioral factors, occupation, and resources of adjustment affect an individual’s quality of life [16]. The degree of individuals’ flexibility is among the factors affecting the quality of life.
Flexibility is defined as the ability of cognitive sets to be adapted according to changing environmental stimuli [17]. Cognitive flexibility means the extent, to which a person is open to experience regarding internal and external experiences. This personality trait determines the reaction of individuals against new experiences [18]. Flexibility requires the ability [19]. Flexible people are curious and their lives are rich in terms of experience. Not only they do not avoid encountering internal and external experiences but also they seek new experiences [20].
Among the effective treatments, interventions to improve the quality of life and increase the amount of psychological flexibility is the Acceptance and Commitment Therapy (ACT). The ACT is a cognitive-behavioral therapy based on functional contextualism. It is rooted in a new theory about language and cognition, which is called the theory of mental relations framework. In the ACT, it is assumed that humans consider many of their own internal feelings, emotions, or thoughts annoying and constantly try to change or discharge these inner experiences. These attempts to control them have been ineffective and contradictorily have resulted in the exacerbation of feelings, emotions, and thoughts that the individual initially tried to avoid [21].
The ACT has 6 central processes that lead to psychological flexibility; the processes include acceptance vs. avoidance, dissonance vs. cognitive blending, self as a context vs. conceptualized self, the relation of the present vs. the overcoming of the past and the conceptualized future, emphasis on values vs. the lack of clarity of values and their relation to them, and the commitment vs. being isolated [22]. In fact, this type of treatment is the main purpose of creating psychological flexibility; that is, the ability to make practical choices among different options that are more appropriate, rather than an action merely to avoid disturbing thoughts, emotions, memories or desires, or actually imposed on an individual [23].
The necessity of the present research is to identify and recognize the psychological problems in students with a learning disorder and taking action regarding their treatment and their problems, which should be considered by families and educators. On the one hand, in spite of the expansion of the present research scope, a few studies have been conducted. As long as there is no comprehensive research on effective methods and techniques for improving the quality of life and psychological flexibility, parents, teachers, and education officials cannot plan properly in this regard. Therefore, in order to prevent further problems, paying attention to these students and doing timely and preventive interventions is necessary. The aim of this study was to determine the efficacy of ACT on the quality of life and psychological flexibility of female junior high school students with learning disorders in Sari, Iran.
2. Materials and Methods
The present quasi-experimental study used a Pre-test-Post-test design with a control group. The statistical population included all female junior high school students with special learning disorders in Sari, who were referred to the learning disorders and counseling centers during the academic year 2018-2019. At first, between the two areas of the city, one district was randomly selected and, then, 60 individuals were selected by the convenience sampling method; next, they were randomly assigned to the experimental and the control groups (30 in the experimental group and 30 in the control group). Based on the effect size of 0.25, alpha of 0.5, and power of 0.85 in the two groups, the minimum number of samples to achieve the desired power, 30 individuals in each group and a total of 60 individuals, was determined. The inclusion criteria include the occurrence of a particular learning disorder (reading and math), female gender, junior high school student, and the absence of other serious psychiatric disorders such as schizophrenia and bipolar disorder. The exclusion criteria included the absences of more than 2 sessions, disabling physical illness, and the provision of incomplete information. Both groups completed the 36-item Short Form health survey (SF-36) and the Cognitive Flexibility Inventory (CFI) of Dennis and Vander Wal before the intervention. The experimental group was, then, subjected to the influence of the independent variable for 8 sessions (120 minutes for each session) and the control group received no training. In order to evaluate the effect of the training, the tests for both groups were completely optional. Before starting and participating in the project, they became familiar with the layout specifications.
The attitudes and beliefs of the individuals were respected. The members of the experimental and control groups were allowed to leave the research project at any stage. In addition, the group members were free to repeat the treatment sessions of the intervention group if they were interested in entering the intervention group only at the end of the plan. All documents, questionnaires, and confidential records were available only to the administrators. The written and informed consent of the parents or legal guardians of all the candidates was taken. The research was not registered in the Iranian Registry of Clinical Trials.
Cognitive Flexibility Inventory-Iranian Version
The CFI is a brief 20-item self-report instrument designed to measure the aspects of cognitive flexibility that enables individuals to challenge and replace the maladaptive thoughts with more adaptive ones. It can be utilized in clinical and non-clinical areas and to assess the individual’s progress in developing flexible thinking in cognitive behavioral therapy for depression and other psychopathological diseases. The CFI was originally developed to measure 3 aspects of cognitive flexibility; a. the tendency to perceive difficult situations as controllable; b. the ability to perceive multiple alternative explanations for life occurrences and human behaviors; c. the ability to generate multiple alternative solutions to difficult situations, but it ended in two factors and demonstrated the adequate levels of validity, reliability, and internal consistency. More specifically, the Cronbach’s alphas for the CFI, control, alternatives, and subscales were 0.91, 0.84, and 0.91, respectively. The 7-week test-retest reliability coefficients for the CFI, control, and alternatives subscales were 0.81, 0.77, and 0.75, respectively [24]. In this study, Cronbach’s alpha of CFI was 0.79.
Cognitive Flexibility Inventory-Iranian Version
The CFI is a brief 20-item self-report instrument designed to measure the aspects of cognitive flexibility that enables individuals to challenge and replace the maladaptive thoughts with more adaptive ones. It can be utilized in clinical and non-clinical areas and to assess the individual’s progress in developing flexible thinking in cognitive behavioral therapy for depression and other psychopathological diseases. The CFI was originally developed to measure 3 aspects of cognitive flexibility; a. the tendency to perceive difficult situations as controllable; b. the ability to perceive multiple alternative explanations for life occurrences and human behaviors; c. the ability to generate multiple alternative solutions to difficult situations, but it ended in two factors and demonstrated the adequate levels of validity, reliability, and internal consistency. More specifically, the Cronbach’s alphas for the CFI, control, alternatives, and subscales were 0.91, 0.84, and 0.91, respectively. The 7-week test-retest reliability coefficients for the CFI, control, and alternatives subscales were 0.81, 0.77, and 0.75, respectively [24]. In this study, Cronbach’s alpha of CFI was 0.79.
The 36-Item Short Form Health Survey
The SF-36 is a general quality of life instrument that measures 8 health-related concepts; physical functioning (10 items), role limitations because of physical problems (4 items), bodily pain (2 items), general health perceptions (5 items), vitality (4 items), social functioning (2 items), role limitations because of emotional problems (3 items), and perceived mental health (5 items). In addition, a single item that provides an indication of perceived change in general health status over a 1-year period (health transition) is also included in the SF-36 [25]. In this study, Cronbach’s alpha of the SF-36 was 0.73.
The intervention program of training ACT was set up based on the ACT in 8 sessions (120 minutes for each session) once a week for 2 months. Table 1 presents the concise content of each session.
3.Results
The Mean±SD age of the experimental group and the control group was 16.51±0.451 and 16.21±0.730 years, respectively. The control and experimental groups were similar in terms of age, the field of study, and educational level (P>0.05).
To evaluate the efficacy of the treatment, the One-Way Analysis of Covariance (ANCOVA) test was used. The results of the ANCOVA test showed that the assumption of the normalization of the data in the traits measured at the error level of 0.05 was determined by the Shapiro Wilk and Kolmogorov-Smirnov tests (P>0.05). Also, the assumption of equality and mean in the Pre-test stage was reviewed and confirmed (P>0.05). The assumption of the homogeneity of the variance of the variable was considered during the study (P>0.05). Also, the linearity assumption of the relationship between the Pre-test-Post-test, Post-test-follow-up, and Pre-test-follow-up at the level of 0.05 was statistically significant (P<0.05). Regarding the homogeneity assumption of the slope of the regression line, all traits were also examined. It implied the confirmation of gradient homogeneity of the regression line; the F value obtained from the interaction between the Pre-test score of the trait and the effect of the group was not significant at the error level of 0.05 (P>0.05). Therefore, considering that the conditions and assumptions of the ANCOVA test were established for each trait, to evaluate the efficacy of ACT therapy, the ANCOVA test was used. Tables 2 and 3 present the results of the treatment.
The SF-36 is a general quality of life instrument that measures 8 health-related concepts; physical functioning (10 items), role limitations because of physical problems (4 items), bodily pain (2 items), general health perceptions (5 items), vitality (4 items), social functioning (2 items), role limitations because of emotional problems (3 items), and perceived mental health (5 items). In addition, a single item that provides an indication of perceived change in general health status over a 1-year period (health transition) is also included in the SF-36 [25]. In this study, Cronbach’s alpha of the SF-36 was 0.73.
The intervention program of training ACT was set up based on the ACT in 8 sessions (120 minutes for each session) once a week for 2 months. Table 1 presents the concise content of each session.
3.Results
The Mean±SD age of the experimental group and the control group was 16.51±0.451 and 16.21±0.730 years, respectively. The control and experimental groups were similar in terms of age, the field of study, and educational level (P>0.05).
To evaluate the efficacy of the treatment, the One-Way Analysis of Covariance (ANCOVA) test was used. The results of the ANCOVA test showed that the assumption of the normalization of the data in the traits measured at the error level of 0.05 was determined by the Shapiro Wilk and Kolmogorov-Smirnov tests (P>0.05). Also, the assumption of equality and mean in the Pre-test stage was reviewed and confirmed (P>0.05). The assumption of the homogeneity of the variance of the variable was considered during the study (P>0.05). Also, the linearity assumption of the relationship between the Pre-test-Post-test, Post-test-follow-up, and Pre-test-follow-up at the level of 0.05 was statistically significant (P<0.05). Regarding the homogeneity assumption of the slope of the regression line, all traits were also examined. It implied the confirmation of gradient homogeneity of the regression line; the F value obtained from the interaction between the Pre-test score of the trait and the effect of the group was not significant at the error level of 0.05 (P>0.05). Therefore, considering that the conditions and assumptions of the ANCOVA test were established for each trait, to evaluate the efficacy of ACT therapy, the ANCOVA test was used. Tables 2 and 3 present the results of the treatment.
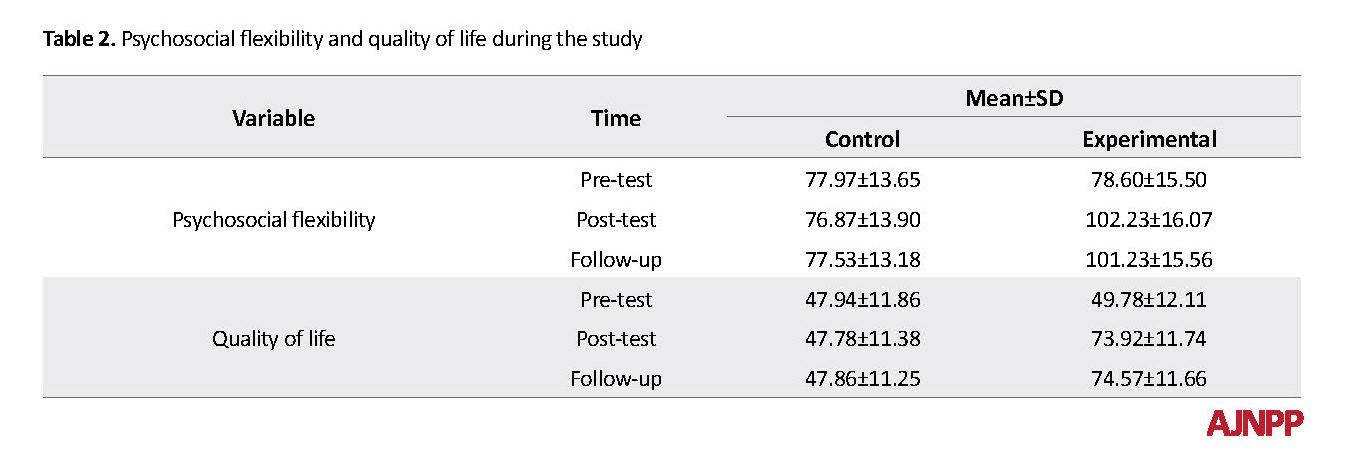
In the Post-test phase, the Pre-test variable as a covariate variable in the model was significant for all variables (P<0.01). The total score of psychosocial flexibility showed that the effect size of the ACT in the total psychosocial flexibility was 0.817. According to the results of the F test in the ANCOVA test and mean values in Table 1, the increasing trend of this variable was significant (P<0.001). The changes in follow-up to Post-test and follow-up to Pre-test were evaluated. The efficacy of the ACT in follow-up to Pre-test was significant (P<0.001) and the effect size was 0.885. In order to determine the stability of the treatment, the follow-up and Post-test were compared. The changes, in this case, were not significant in the two groups (P>0.05). In fact, considering the mean values in Table 1, the groups were stable in the follow-up compared to the Post-test.
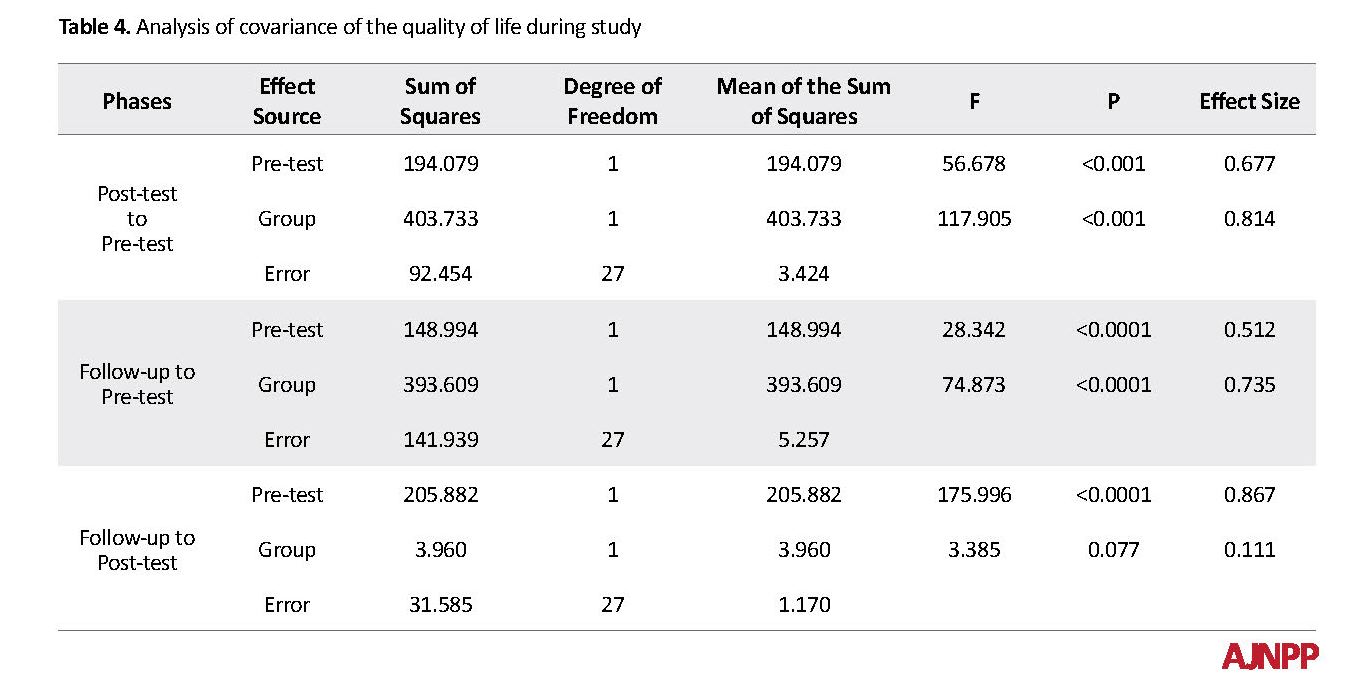
The quality of life in post-test to pre-test of the effect of ACT was 0.814 and according to the results of the F test in the ANCOVA test and the mean values in Table 4, the incremental trend of this variable was significant (P<0.001). The changes in follow-up to the Pre-test also showed that treatment was effective in the follow-up compared to the pre-test (P<0.001) and the effect size was 0.735. In order to determine the stability of the treatment, the follow-up and post-test were compared. The changes in this period were not significant in the two groups (P<0.05). In fact, considering the mean values in Table 1, the groups were stable in the follow-up compared to the post-test.
4. Discussion
The results of this study showed that the level of the total score of psychosocial flexibility was 77.97 and 78.60 in the pre-test of the control and experimental groups, respectively. In the post-test of the control group, this score was changed to 76.87 and in the Post-test of the experimental group, it changed to 102.23. In the experimental group, after the treatment in comparison to before treatment, there was an increase in the pre-treatment score; in the Post-test of the experimental group, it changed from 49.78 to 73.92 and in the follow-up, it changed to 74.57. The changes in the control group showed that the mean was 47.94 in the pre-test, 47.87 in the Post-test, and47.86 in the follow-up. This finding is consistent with the studies of Lappalainen et.al [26] Moazzezi et al. [27], and Clarke et al [28].
In the experimental group, how to improve the state of their life was taught rather than the intellectual and practical avoidance of social thoughts and situations by increasing the acceptance of internal experiences and reaching specific values and goals. In fact, active and effective confrontation with emotions, avoiding evasion, changing attitudes toward themselves and problems, revising goals and values, and ultimately committing to a social goal can be considered the main factors of this method, which improve social compatibility. The ACT helps individuals to identify life tensions (which reduces mental and emotional excitement), copes with stressful resources and being helped when needed and improves social skills and the individual learns to accept and abandon unpleasant experiences of life without attempting to change them. Generally, the ACT helps students with learning disorders learn to become aware of their thoughts and emotions, abandon the previous maladaptive solutions that prevent them from reaching their adaptive goals and values, and get free from self-destructive struggle and improve the psychosocial flexibility.
As another finding of the present study, the quality of life of the experimental group was significantly increased compared to the quality of life of the control group. The results of this study are consistent with the research by Bohlmeijer et al. [29], Arch et al. [30], and other studies that found the efficacy of this treatment in increasing quality of life. In explaining the efficacy of ACT on increasing the quality of life, it is worth noting that this treatment trains the learners to reduce experiential avoidance and acceptance practices and discussions about goals and values. Assessing the effectiveness of measures to achieve them, identifying and focusing on thinking ruminations, as well as relaxing from them, and lacking judgment and responding to unpleasant experiences result in an increase in the quality of life of students.
Each research has its own limitations that can affect its results. The impossibility to control intervening variables such as socio-familial and familial status of students and other individual characteristics, using the convenience sampling method and the effectiveness of treatment on female students were considered the limitations of this study. Based on the findings of this study, it is suggested that in other studies, the other demographic variables should be monitored for further accuracy so that the results can be attributed to the treatment program. In general, given the results of both hypotheses based on the positive effects of ACT on social adjustment and quality of life, it is suggested that this training should be provided in the form of general education through CD or brochure for all students in different stages and should be taught to school advisers.
5. Conclusion
The ACT increased the psychosocial flexibility and quality of life of female junior high school students with learning disorders.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages and signed the informed consent; they were also assured about the confidentiality of their information. Moreover, they were allowed to leave the study whenever they wish and, if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed equally in preparing all parts of the research.
Conflict of interest
The authors have no conflict of interest.
References
Snowling MJ, Hulme C. Annual Research Review: The nature and classification of reading disorders-a commentary on proposals for DSM‐5. Journal of Child Psychology and Psychiatry. 2012; 53(5):593-607. [DOI:10.1111/j.1469-7610.2011.02495.x] [PMID] [PMCID]
Miciak J, Cirino PT, Ahmed Y, Reid E, Vaughn S. Executive functions and response to intervention: Identification of students struggling with reading comprehension. Learning Disability Quarterly. 2019; 42(1):17-31. [DOI:10.1177%2F0731948717749935] [PMID] [PMCID]
Cragg L, Richardson S, Hubber PJ, Keeble S, Gilmore C. When is working memory important for arithmetic? The impact of strategy and age. PloS One. 2017; 12(12):e0188693. [DOI:10.1371/journal.pone.0188693] [PMID] [PMCID]
Gray S, Fox AB, Green S, Alt M, Hogan TP, Petscher Y, Cowan N. Working Memory Profiles of Children with Dyslexia, Developmental Language Disorder, or Both. Journal of Speech, Language, and Hearing Research. 2019; 1-20. [DOI:10.1044/2019_JSLHR-L-18-0148] [PMID] [PMCID]
Compton DL, Fuchs LS, Fuchs D, Lambert W, Hamlett C. The cognitive and academic profiles of reading and mathematics learning disabilities. Journal of Learning Disabilities. 2012; 45(1):79-95. [DOI:10.1177%2F0022219410393012] [PMID] [PMCID]
Freilich R, Shechtman Z. The contribution of art therapy to the social, emotional, and academic adjustment of children with learning disabilities. The Arts in Psychotherapy. 2010; 37(2):97-105. [DOI:10.1016/j.aip.2010.02.003]
Bauminger N, Kimhi-Kind I. Social information processing, security of attachment, and emotion regulation in children with learning disabilities. Journal of Learning Disabilities. 2008; 41(4):315-32. [DOI:10.1177%2F0022219408316095] [PMID]
Løhre A, Moksnes UK, Lillefjell M. Gender differences in predictors of school wellbeing? Health Education Journal. 2014; 73(1):90-100. [DOI:10.1177%2F0017896912470822]
Slaughter V, Imuta K, Peterson CC, Henry JD. Meta‐analysis of theory of mind and peer popularity in the preschool and early school years. Child Development. 2015; 86(4):1159-74. [DOI:10.1111/cdev.12372] [PMID]
Cooley JL, Fite PJ, Rubens SL, Tunno AM. Peer victimization, depressive symptoms, and rule-breaking behavior in adolescence: The moderating role of peer social support. Journal of Psychopathology and Behavioral Assessment. 2015; 37(3):512-22. [DOI:10.1007/s10862-014-9473-7]
Sideridis GD. International approaches to learning disabilities: More alike or more different? Learning Disabilities Research & Practice. 2007; 22(3):210-5. [DOI:10.1111/j.1540-5826.2007.00249.x]
Nelson JM, Harwood H. Learning disabilities and anxiety: A meta-analysis. Journal of Learning Disabilities. 2011; 44(1):3-17. [DOI:10.1177%2F0022219409359939] [PMID]
Gallegos J, Langley A, Villegas D. Anxiety, depression, and coping skills among Mexican school children: A comparison of students with and without learning disabilities. Learning Disability Quarterly. 2012; 35(1):54-61. [DOI:10.1177%2F0731948711428772] [PMID] [PMCID]
Kiuru N, Leskinen E, Nurmi JE, Salmela-Aro K. Depressive symptoms during adolescence: Do learning difficulties matter? International Journal of Behavioral Development. 2011; 35(4):298-306. [DOI:10.1177%2F0165025410396764]
An BP. The role of academic motivation and engagement on the relationship between dual enrollment and academic performance. The Journal of Higher Education. 2015; 86(1):98-126. [DOI:10.1080/00221546.2015.11777358]
Mullender‐Wijnsma MJ, Hartman E, de Greeff JW, Bosker RJ, Doolaard S, Visscher C. Improving academic performance of school‐age children by physical activity in the classroom: 1‐year program evaluation. Journal of School Health. 2015; 85(6):365-71. [DOI:10.1111/josh.12259] [PMID]
Hungerford A, Wait SK, Fritz AM, Clements CM. Exposure to intimate partner violence and children’s psychological adjustment, cognitive functioning, and social competence: A review. Aggression and Violent Behavior. 2012; 17(4):373-82. [DOI:10.1016/j.avb.2012.04.002]
Leichtentritt J, Shechtman Z. Children with and without learning disabilities: A comparison of processes and outcomes following group counseling. Journal of Learning Disabilities. 2010; 43(2):169-79. [DOI:10.1177%2F0022219409345008] [PMID]
Scanlon D. Specific learning disability and its newest definition: Which is comprehensive? And which is insufficient? Journal of Learning Disabilities. 2013; 46(1):26-33. [DOI:10.1177%2F0022219412464342] [PMID]
Hopkins IM, Gower MW, Perez TA, Smith DS, Amthor FR, Wimsatt FC, Biasini FJ. Avatar assistant: improving social skills in students with an ASD through a computer-based intervention. Journal of Autism and Developmental Disorders. 2011; 41(11):1543-55. [DOI:10.1007/s10803-011-1179-z] [PMID]
Pich J, Bibiloni MD, Pons A, Tur JA. Weight self-regulation process in adolescence: the relationship between control weight attitudes, behaviors, and body weight status. Frontiers in Nutrition. 2015; 2:14. [DOI:10.3389/fnut.2015.00014] [PMID] [PMCID]
Hayes SC, Levin ME, Plumb-Vilardaga J, Villatte JL, Pistorello J. Acceptance and commitment therapy and contextual behavioral science: Examining the progress of a distinctive model of behavioral and cognitive therapy. Behavior Therapy. 2013; 44(2):180-98. [DOI:10.1016/j.beth.2009.08.002] [PMID] [PMCID]
Bricker JB, Mull KE, Kientz JA, Vilardaga R, Mercer LD, Akioka KJ, Heffner JL. Randomized, controlled pilot trial of a smartphone app for smoking cessation using acceptance and commitment therapy. Drug and Alcohol Dependence. 2014; 143:87-94. [DOI:10.1016/j.drugalcdep.2014.07.006] [PMID] [PMCID]
Dennis JP, Vander Wal JS. The cognitive flexibility inventory: Instrument development and estimates of reliability and validity. Cognitive Therapy and Research. 2010; 34(3):241-53. [DOI:10.1007/s10608-009-9276-4]
Su CT, Ng HS, Yang AL, Lin CY. Psychometric evaluation of the Short Form 36 Health Survey (SF-36) and the World Health Organization Quality of Life Scale Brief Version (WHOQOL-BREF) for patients with schizophrenia. Psychological Assessment. 2014; 26(3):980. [DOI:10.1037/a0036764] [PMID]
Lappalainen P, Granlund A, Siltanen S, Ahonen S, Vitikainen M, Tolvanen A, Lappalainen R. ACT Internet-based vs face-to-face? A randomized controlled trial of two ways to deliver Acceptance and Commitment Therapy for depressive symptoms: An 18-month follow-up. Behaviour Research and Therapy. 2014; 61:43-54. [DOI:10.1016/j.brat.2014.07.006] [PMID]
Moazzezi M, Moghanloo VA, Moghanloo RA, Pishvaei M. Impact of acceptance and commitment therapy on perceived stress and special health self-efficacy in seven to fifteen-year-old children with diabetes mellitus. Iranian Journal of Psychiatry and Dehavioral Sciences. 2015; 9(2). [DOI:10.17795/ijpbs956] [PMID] [PMCID]
Clarke S, Kingston J, James K, Bolderston H, Remington B. Acceptance and Commitment Therapy group for treatment-resistant participants: A randomized controlled trial. Journal of Contextual Behavioral Science. 2014; 3(3):179-88. [DOI:10.1016/j.jcbs.2014.04.005]
Bohlmeijer ET, Fledderus M, Rokx TA, Pieterse ME. Efficacy of an early intervention based on acceptance and commitment therapy for adults with depressive symptomatology: Evaluation in a randomized controlled trial. Behaviour research and therapy. 2011; 49(1):62-7. [DOI:10.1016/j.jpsychores.2009.10.005] [PMID]
Arch JJ, Eifert GH, Davies C, Vilardaga JC, Rose RD, Craske MG. Randomized clinical trial of cognitive behavioral therapy (CBT) versus Acceptance and Commitment Therapy (ACT) for mixed anxiety disorders. Journal of consulting and clinical psychology. 2012; 80(5):750. [DOI:10.1037/a0028310] [PMID] [PMCID]
4. Discussion
The results of this study showed that the level of the total score of psychosocial flexibility was 77.97 and 78.60 in the pre-test of the control and experimental groups, respectively. In the post-test of the control group, this score was changed to 76.87 and in the Post-test of the experimental group, it changed to 102.23. In the experimental group, after the treatment in comparison to before treatment, there was an increase in the pre-treatment score; in the Post-test of the experimental group, it changed from 49.78 to 73.92 and in the follow-up, it changed to 74.57. The changes in the control group showed that the mean was 47.94 in the pre-test, 47.87 in the Post-test, and47.86 in the follow-up. This finding is consistent with the studies of Lappalainen et.al [26] Moazzezi et al. [27], and Clarke et al [28].
In the experimental group, how to improve the state of their life was taught rather than the intellectual and practical avoidance of social thoughts and situations by increasing the acceptance of internal experiences and reaching specific values and goals. In fact, active and effective confrontation with emotions, avoiding evasion, changing attitudes toward themselves and problems, revising goals and values, and ultimately committing to a social goal can be considered the main factors of this method, which improve social compatibility. The ACT helps individuals to identify life tensions (which reduces mental and emotional excitement), copes with stressful resources and being helped when needed and improves social skills and the individual learns to accept and abandon unpleasant experiences of life without attempting to change them. Generally, the ACT helps students with learning disorders learn to become aware of their thoughts and emotions, abandon the previous maladaptive solutions that prevent them from reaching their adaptive goals and values, and get free from self-destructive struggle and improve the psychosocial flexibility.
As another finding of the present study, the quality of life of the experimental group was significantly increased compared to the quality of life of the control group. The results of this study are consistent with the research by Bohlmeijer et al. [29], Arch et al. [30], and other studies that found the efficacy of this treatment in increasing quality of life. In explaining the efficacy of ACT on increasing the quality of life, it is worth noting that this treatment trains the learners to reduce experiential avoidance and acceptance practices and discussions about goals and values. Assessing the effectiveness of measures to achieve them, identifying and focusing on thinking ruminations, as well as relaxing from them, and lacking judgment and responding to unpleasant experiences result in an increase in the quality of life of students.
Each research has its own limitations that can affect its results. The impossibility to control intervening variables such as socio-familial and familial status of students and other individual characteristics, using the convenience sampling method and the effectiveness of treatment on female students were considered the limitations of this study. Based on the findings of this study, it is suggested that in other studies, the other demographic variables should be monitored for further accuracy so that the results can be attributed to the treatment program. In general, given the results of both hypotheses based on the positive effects of ACT on social adjustment and quality of life, it is suggested that this training should be provided in the form of general education through CD or brochure for all students in different stages and should be taught to school advisers.
5. Conclusion
The ACT increased the psychosocial flexibility and quality of life of female junior high school students with learning disorders.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages and signed the informed consent; they were also assured about the confidentiality of their information. Moreover, they were allowed to leave the study whenever they wish and, if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed equally in preparing all parts of the research.
Conflict of interest
The authors have no conflict of interest.
References
Snowling MJ, Hulme C. Annual Research Review: The nature and classification of reading disorders-a commentary on proposals for DSM‐5. Journal of Child Psychology and Psychiatry. 2012; 53(5):593-607. [DOI:10.1111/j.1469-7610.2011.02495.x] [PMID] [PMCID]
Miciak J, Cirino PT, Ahmed Y, Reid E, Vaughn S. Executive functions and response to intervention: Identification of students struggling with reading comprehension. Learning Disability Quarterly. 2019; 42(1):17-31. [DOI:10.1177%2F0731948717749935] [PMID] [PMCID]
Cragg L, Richardson S, Hubber PJ, Keeble S, Gilmore C. When is working memory important for arithmetic? The impact of strategy and age. PloS One. 2017; 12(12):e0188693. [DOI:10.1371/journal.pone.0188693] [PMID] [PMCID]
Gray S, Fox AB, Green S, Alt M, Hogan TP, Petscher Y, Cowan N. Working Memory Profiles of Children with Dyslexia, Developmental Language Disorder, or Both. Journal of Speech, Language, and Hearing Research. 2019; 1-20. [DOI:10.1044/2019_JSLHR-L-18-0148] [PMID] [PMCID]
Compton DL, Fuchs LS, Fuchs D, Lambert W, Hamlett C. The cognitive and academic profiles of reading and mathematics learning disabilities. Journal of Learning Disabilities. 2012; 45(1):79-95. [DOI:10.1177%2F0022219410393012] [PMID] [PMCID]
Freilich R, Shechtman Z. The contribution of art therapy to the social, emotional, and academic adjustment of children with learning disabilities. The Arts in Psychotherapy. 2010; 37(2):97-105. [DOI:10.1016/j.aip.2010.02.003]
Bauminger N, Kimhi-Kind I. Social information processing, security of attachment, and emotion regulation in children with learning disabilities. Journal of Learning Disabilities. 2008; 41(4):315-32. [DOI:10.1177%2F0022219408316095] [PMID]
Løhre A, Moksnes UK, Lillefjell M. Gender differences in predictors of school wellbeing? Health Education Journal. 2014; 73(1):90-100. [DOI:10.1177%2F0017896912470822]
Slaughter V, Imuta K, Peterson CC, Henry JD. Meta‐analysis of theory of mind and peer popularity in the preschool and early school years. Child Development. 2015; 86(4):1159-74. [DOI:10.1111/cdev.12372] [PMID]
Cooley JL, Fite PJ, Rubens SL, Tunno AM. Peer victimization, depressive symptoms, and rule-breaking behavior in adolescence: The moderating role of peer social support. Journal of Psychopathology and Behavioral Assessment. 2015; 37(3):512-22. [DOI:10.1007/s10862-014-9473-7]
Sideridis GD. International approaches to learning disabilities: More alike or more different? Learning Disabilities Research & Practice. 2007; 22(3):210-5. [DOI:10.1111/j.1540-5826.2007.00249.x]
Nelson JM, Harwood H. Learning disabilities and anxiety: A meta-analysis. Journal of Learning Disabilities. 2011; 44(1):3-17. [DOI:10.1177%2F0022219409359939] [PMID]
Gallegos J, Langley A, Villegas D. Anxiety, depression, and coping skills among Mexican school children: A comparison of students with and without learning disabilities. Learning Disability Quarterly. 2012; 35(1):54-61. [DOI:10.1177%2F0731948711428772] [PMID] [PMCID]
Kiuru N, Leskinen E, Nurmi JE, Salmela-Aro K. Depressive symptoms during adolescence: Do learning difficulties matter? International Journal of Behavioral Development. 2011; 35(4):298-306. [DOI:10.1177%2F0165025410396764]
An BP. The role of academic motivation and engagement on the relationship between dual enrollment and academic performance. The Journal of Higher Education. 2015; 86(1):98-126. [DOI:10.1080/00221546.2015.11777358]
Mullender‐Wijnsma MJ, Hartman E, de Greeff JW, Bosker RJ, Doolaard S, Visscher C. Improving academic performance of school‐age children by physical activity in the classroom: 1‐year program evaluation. Journal of School Health. 2015; 85(6):365-71. [DOI:10.1111/josh.12259] [PMID]
Hungerford A, Wait SK, Fritz AM, Clements CM. Exposure to intimate partner violence and children’s psychological adjustment, cognitive functioning, and social competence: A review. Aggression and Violent Behavior. 2012; 17(4):373-82. [DOI:10.1016/j.avb.2012.04.002]
Leichtentritt J, Shechtman Z. Children with and without learning disabilities: A comparison of processes and outcomes following group counseling. Journal of Learning Disabilities. 2010; 43(2):169-79. [DOI:10.1177%2F0022219409345008] [PMID]
Scanlon D. Specific learning disability and its newest definition: Which is comprehensive? And which is insufficient? Journal of Learning Disabilities. 2013; 46(1):26-33. [DOI:10.1177%2F0022219412464342] [PMID]
Hopkins IM, Gower MW, Perez TA, Smith DS, Amthor FR, Wimsatt FC, Biasini FJ. Avatar assistant: improving social skills in students with an ASD through a computer-based intervention. Journal of Autism and Developmental Disorders. 2011; 41(11):1543-55. [DOI:10.1007/s10803-011-1179-z] [PMID]
Pich J, Bibiloni MD, Pons A, Tur JA. Weight self-regulation process in adolescence: the relationship between control weight attitudes, behaviors, and body weight status. Frontiers in Nutrition. 2015; 2:14. [DOI:10.3389/fnut.2015.00014] [PMID] [PMCID]
Hayes SC, Levin ME, Plumb-Vilardaga J, Villatte JL, Pistorello J. Acceptance and commitment therapy and contextual behavioral science: Examining the progress of a distinctive model of behavioral and cognitive therapy. Behavior Therapy. 2013; 44(2):180-98. [DOI:10.1016/j.beth.2009.08.002] [PMID] [PMCID]
Bricker JB, Mull KE, Kientz JA, Vilardaga R, Mercer LD, Akioka KJ, Heffner JL. Randomized, controlled pilot trial of a smartphone app for smoking cessation using acceptance and commitment therapy. Drug and Alcohol Dependence. 2014; 143:87-94. [DOI:10.1016/j.drugalcdep.2014.07.006] [PMID] [PMCID]
Dennis JP, Vander Wal JS. The cognitive flexibility inventory: Instrument development and estimates of reliability and validity. Cognitive Therapy and Research. 2010; 34(3):241-53. [DOI:10.1007/s10608-009-9276-4]
Su CT, Ng HS, Yang AL, Lin CY. Psychometric evaluation of the Short Form 36 Health Survey (SF-36) and the World Health Organization Quality of Life Scale Brief Version (WHOQOL-BREF) for patients with schizophrenia. Psychological Assessment. 2014; 26(3):980. [DOI:10.1037/a0036764] [PMID]
Lappalainen P, Granlund A, Siltanen S, Ahonen S, Vitikainen M, Tolvanen A, Lappalainen R. ACT Internet-based vs face-to-face? A randomized controlled trial of two ways to deliver Acceptance and Commitment Therapy for depressive symptoms: An 18-month follow-up. Behaviour Research and Therapy. 2014; 61:43-54. [DOI:10.1016/j.brat.2014.07.006] [PMID]
Moazzezi M, Moghanloo VA, Moghanloo RA, Pishvaei M. Impact of acceptance and commitment therapy on perceived stress and special health self-efficacy in seven to fifteen-year-old children with diabetes mellitus. Iranian Journal of Psychiatry and Dehavioral Sciences. 2015; 9(2). [DOI:10.17795/ijpbs956] [PMID] [PMCID]
Clarke S, Kingston J, James K, Bolderston H, Remington B. Acceptance and Commitment Therapy group for treatment-resistant participants: A randomized controlled trial. Journal of Contextual Behavioral Science. 2014; 3(3):179-88. [DOI:10.1016/j.jcbs.2014.04.005]
Bohlmeijer ET, Fledderus M, Rokx TA, Pieterse ME. Efficacy of an early intervention based on acceptance and commitment therapy for adults with depressive symptomatology: Evaluation in a randomized controlled trial. Behaviour research and therapy. 2011; 49(1):62-7. [DOI:10.1016/j.jpsychores.2009.10.005] [PMID]
Arch JJ, Eifert GH, Davies C, Vilardaga JC, Rose RD, Craske MG. Randomized clinical trial of cognitive behavioral therapy (CBT) versus Acceptance and Commitment Therapy (ACT) for mixed anxiety disorders. Journal of consulting and clinical psychology. 2012; 80(5):750. [DOI:10.1037/a0028310] [PMID] [PMCID]
Article Type: Research Article |
Subject:
Learning and Memory, Dementia, Alzheimer
Received: 2019/07/15 | Accepted: 2019/08/28 | Published: 2019/09/17
Received: 2019/07/15 | Accepted: 2019/08/28 | Published: 2019/09/17
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Hamadan University of Medical Sciences.
Published by UMSHA Press
Journal Tel: +989025126654
Publisher Tel: +985136014377
Website: http://ajnpp.umsha.ac.ir
Email: avicennajnpp[at]gmail.com
