

Volume 4, Issue 4 (November 2017)
Avicenna J Neuro Psycho Physiology 2017, 4(4): 137-144 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Karami-Matin B, Mirzaei-Alavijeh M, Najafi F, Jalilian F. Psychometric Analysis of the Cultural Competence Scale in Iranian Healthcare Providers. Avicenna J Neuro Psycho Physiology 2017; 4 (4) :137-144
URL: http://ajnpp.umsha.ac.ir/article-1-110-en.html
URL: http://ajnpp.umsha.ac.ir/article-1-110-en.html



1- Research Center for Environmental Determinants of Health, Kermanshah University of Medical Sciences, Kermanshah, Iran
2- Social Development and Health Promotion Research Center, Kermanshah University of Medical Sciences, Kermanshah, Iran
3- Research Center for Environmental Determinants of Health, Kermanshah University of Medical Sciences, Kermanshah, Iran , f_jalilian@yahoo.com
2- Social Development and Health Promotion Research Center, Kermanshah University of Medical Sciences, Kermanshah, Iran
3- Research Center for Environmental Determinants of Health, Kermanshah University of Medical Sciences, Kermanshah, Iran , f_jalilian@yahoo.com
Full-Text [PDF 694 kb]
(643 Downloads)
| Abstract (HTML) (1860 Views)

Full-Text: (1004 Views)
1. Introduction
Healthcare is one of the most basic human rights that should be equally accessible to all individuals [1]. Many countries not only provide healthcare but also pay special attention to other aspects of health promotion like equality and seek to reduce healthcare inequity [2]. Whitehead has defined healthcare inequities as unnecessary and avoidable differences that are considered unfair and inaccurate [3]. The National Institutes of Health also defined health inequalities as the differences in the incidence, prevalence, mortality, and burden of diseases and other adverse health conditions among different population groups [4]. Despite improving health and overall health indicators, health inequalities have increased over the past decades. Some studies have revealed racial and ethnic inequalities in the quality of healthcare [5, 6].
“CC” can be an effective approach in reducing ethnic and racial inequalities in healthcare [7]. Research has recognized CC as an effective strategy for reducing health inequalities and improving the quality and accessibility of health services [8-11]. Additionally, CC can improve patient adherence to healthcare programs [12]. There are several definitions of CC; e.g. “the ability to establish effective interpersonal relationships” or “the ability to work cross-culturally” [13, 14]. The American Association for Health Education defines CC as the ability of an individual to understand and respect values, attitudes, and cultural mores, to consider and respond appropriately in planning, implementing, and evaluating health promotion programs [4]. According to Davis and Rankin, CC defines differences between successful and unsuccessful programs [15].
Assessing cultural competence in healthcare providers, especially in societies with cultural diversity is important. It helps in developing, implementing and evaluating health promotion programs to improve CC by valid and reliable scales [16-20]. However, awareness of the existing conditions and determinants affecting this issue is necessary for planning health promotion programs [21-24]. Therefore, to carry out research, there is a need for a standard scientific questionnaire [25, 26]. There is a lack of access to such questionnaires that address the cultural characteristics of Iranian society. Thus, this study aimed to investigate the psychometric properties of the Cultural Competence Scale (CCS) among healthcare providers in Kermanshah, Iran.
2. Materials and Methods
This cross-sectional study was conducted among 192 healthcare providers in Kermanshah City, Iran, in 2018. Kermanshah Province is located in the west of Iran with a high cultural diversity, where different ethnicities such as Persian, Kurdish, Turkish, etc. live together. Moreover, Kermanshah Province has a great variety of religious views. Most of the inhabitants of Kermanshah are Shia Muslims; however, there are minorities, such as Sunni Muslims, Yarsanism, Christianity, Jewish, and so on [27].
Investigators disregarded the assessment of CC in health service providers in Iran; thus, the items which assessed the cultural competency were derived from the scales of cultural competency [16-20]. To facilitate the study participants’ responses to the items, all items were standardized to a 5-point Likert-Type Scale, ranging from 1 (strongly disagree) to 5 (strongly agree). The questionnaire was translated into Persian by two professional translators. It was back-translated to English after consulting with some professors and a third person with proficiency in both languages. After being synchronized with the main form and removing the problems, the questionnaire was translated back to English to examine its validity and reliability.
The assessed background variables included age (years), gender (male/ female), marital status (married/ single), educational level (Associate degree/ BSc./ MSc./ MD.), job history (years), and being native and nonnative of Kermanshah (yes/ no). The items which assessed the CC constructs were derived from the scales of cultural competency [16-20]. There were 24 items which measured the 5 constructs of cultural skill, cultural awareness, cultural desire, cultural encounters, and cultural behavior. Eight items measured cultural skill (e.g. I can use appropriate communication skills when dealing with clients from different cultural backgrounds). Five items measured the cultural awareness (e.g. I know the non-verbal behaviors among different ethnic groups in the region). Five items measured the cultural desire (e.g. I tend to work with different ethnic groups from different cultural backgrounds). The cultural encounter was measured by 4 items (e.g. When I am faced with different cultures, I usually do not feel useful). In addition, the cultural behavior was measured by two items (e.g. I don’t have any prejudices; that ethnicity has healthier behaviors) to different ethnicities living in a district for health care).
The number of samples recommended for factor analysis is 5-10 subjects per every item of the scale [28]. Considering the number of items (it was 24 in the preliminary questionnaire), 8 samples have been considered for each item; therefore, a total of 192 samples were randomly selected. The study participants were the male and female healthcare providers from 8 health centers in Kermanshah. The health centers of Kermanshah were considered as cluster and were selected by simple random sampling method with probability proportional to size in each cluster. Data collection was performed in a self-report manner. Of the 192 samples, 184 (95.8%) signed the consent form and voluntarily agreed to participate in the study.
The inclusion criteria were the participants’ knowledge about the objectives of the study, consent to participate in the study and work as a healthcare provider at Kermanshah health centers. Incomplete questionnaires were excluded from the study. The Research Ethics Committee at Deputy of Research of the Kermanshah University of Medical Sciences (KUMS.REC.1394.448) had approved the study protocol and had monitored the research process. Furthermore, the study participants were provided with the participant information statement and signed the written informed consent forms. Their personal information was kept confidential. The psychometric assessment of the questionnaire was performed by investigating the validity of the questionnaire using face, content, and constructs validities.
The first qualitative method measured the difficulty, proportionality, and ambiguity of the items in 15 healthcare providers who were matched with the participants of the main study and their response was applied in the questionnaire. Additionally, the item impact was investigated in quantitative methods; and the items of ≤1.5 value were excluded. For evaluating content validity, experts panel was used, including health education, epidemiology, health management, psychology, and health policy specialists. According to the Lawshe’s table and a number of experts (10 persons), the minimum values for Content Validity Ratio (CVR) and Content Validity Index (CVI) were 0.62 and 0.79, respectively [27]. In this section, experts were asked about essentiality, usefulness, and necessity, reflecting the relevant field as well as clarity, briefness and cultural appropriateness of the items.
Classical Item Analysis (CIA) was used to assess construct validity. In the CIA method, mean, standard deviation and Corrected Item-Total Correlation (CITC) of each item was calculated. Exploratory Factor Analysis (EFA) with varimax rotation by using factor loadings of 0.40 was used to allocate items and to determine the degree to which this factor structure replicated the original. The Kaiser-Meyer-Olkin (KMO) test measured the sampling adequacy. The homoscedasticity or homogeneity of variances was evaluated using Bartlett’s test. Scree plot was used to confirm the strengths of exploratory agents. To determine agents, the value was considered as ≥1.3. The reliability of the questionnaire was assessed by examining its internal consistency via Cronbach’s α coefficient. Considering Cronbach’s α coefficient, a threshold of 0.70 was acceptable [29]. The collected data were analyzed by SPSS.
3. Results
The Mean±SD age of respondents was 36.96±7.97 years (age range: 22-54 y). The Mean±SD job history of study participants was 12.32±8.03 years, ranging from 1 to 30 years. A total of 66.8% of the study participants were female, and 33.2% were male. Moreover, 72.8% were married and 27.2% were single. Approximately 18.5%, 56.5%, 14.7%, and 10.3% of the respondents had an Associate degree, BSc, MSc, and MD, respectively. In addition, 92.9% of the study participants were indigenous to Kermanshah Province. No items were deleted with accordance to the obtained face validity results. In terms of content validity, all the items had acceptable validity ratio and index of more than 0.62 and 0.79, respectively.
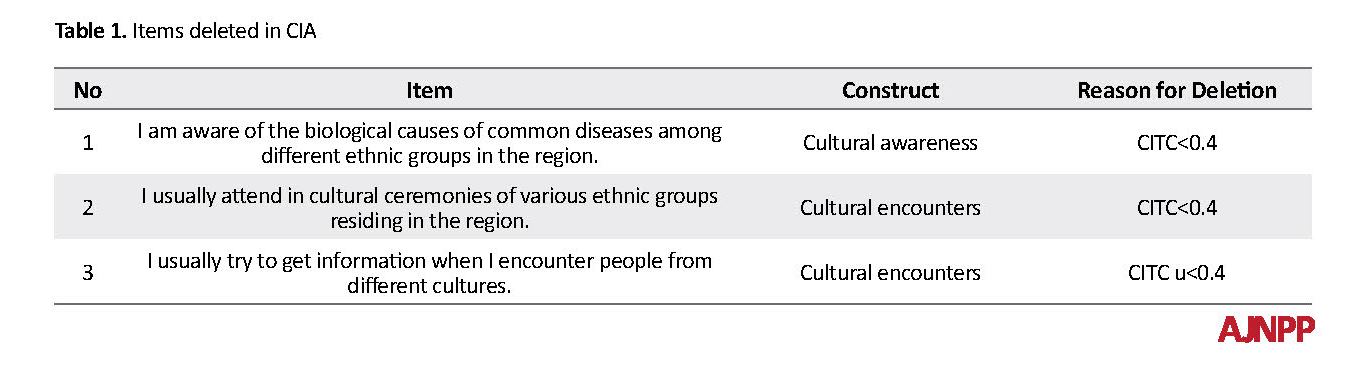
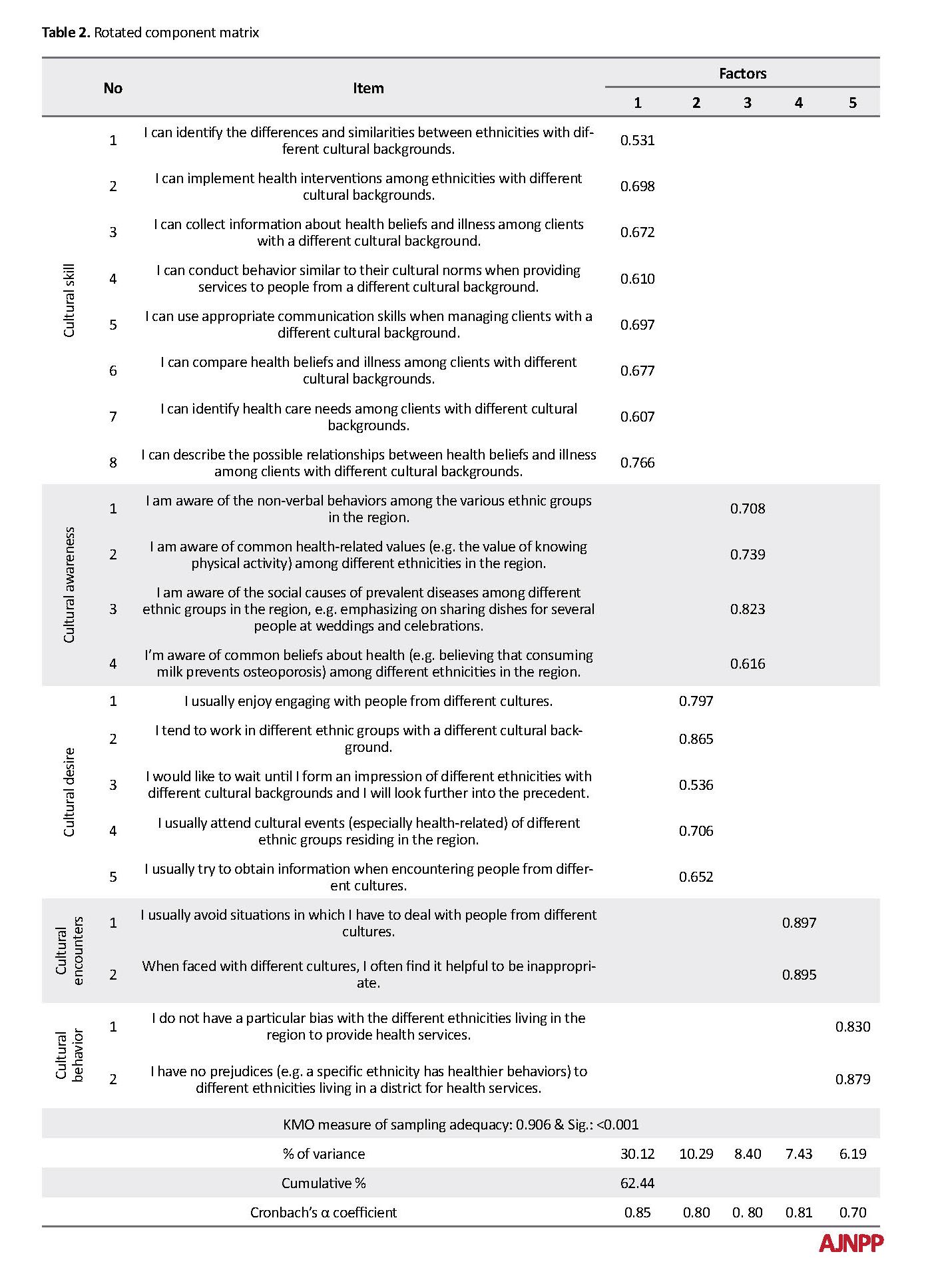
One item of cultural awareness and two items of cultural encounters were eliminated because of CITC<0.4 (Table 1). A total of 21 items entered the exploratory EFA. KMO was equal to 0.906, and Bartlett’s test was also significant at an acceptable level (P<0.001); therefore, the achieved data were appropriate for EFA. Five factors were extracted according to eigenvalues >1 and factors loads of ≥0.4. Overall five factors of cultural skill, cultural awareness, cultural desire, cultural encounters, and cultural behavior described 62.44 % of the assumed model (Table 2).
Healthcare is one of the most basic human rights that should be equally accessible to all individuals [1]. Many countries not only provide healthcare but also pay special attention to other aspects of health promotion like equality and seek to reduce healthcare inequity [2]. Whitehead has defined healthcare inequities as unnecessary and avoidable differences that are considered unfair and inaccurate [3]. The National Institutes of Health also defined health inequalities as the differences in the incidence, prevalence, mortality, and burden of diseases and other adverse health conditions among different population groups [4]. Despite improving health and overall health indicators, health inequalities have increased over the past decades. Some studies have revealed racial and ethnic inequalities in the quality of healthcare [5, 6].
“CC” can be an effective approach in reducing ethnic and racial inequalities in healthcare [7]. Research has recognized CC as an effective strategy for reducing health inequalities and improving the quality and accessibility of health services [8-11]. Additionally, CC can improve patient adherence to healthcare programs [12]. There are several definitions of CC; e.g. “the ability to establish effective interpersonal relationships” or “the ability to work cross-culturally” [13, 14]. The American Association for Health Education defines CC as the ability of an individual to understand and respect values, attitudes, and cultural mores, to consider and respond appropriately in planning, implementing, and evaluating health promotion programs [4]. According to Davis and Rankin, CC defines differences between successful and unsuccessful programs [15].
Assessing cultural competence in healthcare providers, especially in societies with cultural diversity is important. It helps in developing, implementing and evaluating health promotion programs to improve CC by valid and reliable scales [16-20]. However, awareness of the existing conditions and determinants affecting this issue is necessary for planning health promotion programs [21-24]. Therefore, to carry out research, there is a need for a standard scientific questionnaire [25, 26]. There is a lack of access to such questionnaires that address the cultural characteristics of Iranian society. Thus, this study aimed to investigate the psychometric properties of the Cultural Competence Scale (CCS) among healthcare providers in Kermanshah, Iran.
2. Materials and Methods
This cross-sectional study was conducted among 192 healthcare providers in Kermanshah City, Iran, in 2018. Kermanshah Province is located in the west of Iran with a high cultural diversity, where different ethnicities such as Persian, Kurdish, Turkish, etc. live together. Moreover, Kermanshah Province has a great variety of religious views. Most of the inhabitants of Kermanshah are Shia Muslims; however, there are minorities, such as Sunni Muslims, Yarsanism, Christianity, Jewish, and so on [27].
Investigators disregarded the assessment of CC in health service providers in Iran; thus, the items which assessed the cultural competency were derived from the scales of cultural competency [16-20]. To facilitate the study participants’ responses to the items, all items were standardized to a 5-point Likert-Type Scale, ranging from 1 (strongly disagree) to 5 (strongly agree). The questionnaire was translated into Persian by two professional translators. It was back-translated to English after consulting with some professors and a third person with proficiency in both languages. After being synchronized with the main form and removing the problems, the questionnaire was translated back to English to examine its validity and reliability.
The assessed background variables included age (years), gender (male/ female), marital status (married/ single), educational level (Associate degree/ BSc./ MSc./ MD.), job history (years), and being native and nonnative of Kermanshah (yes/ no). The items which assessed the CC constructs were derived from the scales of cultural competency [16-20]. There were 24 items which measured the 5 constructs of cultural skill, cultural awareness, cultural desire, cultural encounters, and cultural behavior. Eight items measured cultural skill (e.g. I can use appropriate communication skills when dealing with clients from different cultural backgrounds). Five items measured the cultural awareness (e.g. I know the non-verbal behaviors among different ethnic groups in the region). Five items measured the cultural desire (e.g. I tend to work with different ethnic groups from different cultural backgrounds). The cultural encounter was measured by 4 items (e.g. When I am faced with different cultures, I usually do not feel useful). In addition, the cultural behavior was measured by two items (e.g. I don’t have any prejudices; that ethnicity has healthier behaviors) to different ethnicities living in a district for health care).
The number of samples recommended for factor analysis is 5-10 subjects per every item of the scale [28]. Considering the number of items (it was 24 in the preliminary questionnaire), 8 samples have been considered for each item; therefore, a total of 192 samples were randomly selected. The study participants were the male and female healthcare providers from 8 health centers in Kermanshah. The health centers of Kermanshah were considered as cluster and were selected by simple random sampling method with probability proportional to size in each cluster. Data collection was performed in a self-report manner. Of the 192 samples, 184 (95.8%) signed the consent form and voluntarily agreed to participate in the study.
The inclusion criteria were the participants’ knowledge about the objectives of the study, consent to participate in the study and work as a healthcare provider at Kermanshah health centers. Incomplete questionnaires were excluded from the study. The Research Ethics Committee at Deputy of Research of the Kermanshah University of Medical Sciences (KUMS.REC.1394.448) had approved the study protocol and had monitored the research process. Furthermore, the study participants were provided with the participant information statement and signed the written informed consent forms. Their personal information was kept confidential. The psychometric assessment of the questionnaire was performed by investigating the validity of the questionnaire using face, content, and constructs validities.
The first qualitative method measured the difficulty, proportionality, and ambiguity of the items in 15 healthcare providers who were matched with the participants of the main study and their response was applied in the questionnaire. Additionally, the item impact was investigated in quantitative methods; and the items of ≤1.5 value were excluded. For evaluating content validity, experts panel was used, including health education, epidemiology, health management, psychology, and health policy specialists. According to the Lawshe’s table and a number of experts (10 persons), the minimum values for Content Validity Ratio (CVR) and Content Validity Index (CVI) were 0.62 and 0.79, respectively [27]. In this section, experts were asked about essentiality, usefulness, and necessity, reflecting the relevant field as well as clarity, briefness and cultural appropriateness of the items.
Classical Item Analysis (CIA) was used to assess construct validity. In the CIA method, mean, standard deviation and Corrected Item-Total Correlation (CITC) of each item was calculated. Exploratory Factor Analysis (EFA) with varimax rotation by using factor loadings of 0.40 was used to allocate items and to determine the degree to which this factor structure replicated the original. The Kaiser-Meyer-Olkin (KMO) test measured the sampling adequacy. The homoscedasticity or homogeneity of variances was evaluated using Bartlett’s test. Scree plot was used to confirm the strengths of exploratory agents. To determine agents, the value was considered as ≥1.3. The reliability of the questionnaire was assessed by examining its internal consistency via Cronbach’s α coefficient. Considering Cronbach’s α coefficient, a threshold of 0.70 was acceptable [29]. The collected data were analyzed by SPSS.
3. Results
The Mean±SD age of respondents was 36.96±7.97 years (age range: 22-54 y). The Mean±SD job history of study participants was 12.32±8.03 years, ranging from 1 to 30 years. A total of 66.8% of the study participants were female, and 33.2% were male. Moreover, 72.8% were married and 27.2% were single. Approximately 18.5%, 56.5%, 14.7%, and 10.3% of the respondents had an Associate degree, BSc, MSc, and MD, respectively. In addition, 92.9% of the study participants were indigenous to Kermanshah Province. No items were deleted with accordance to the obtained face validity results. In terms of content validity, all the items had acceptable validity ratio and index of more than 0.62 and 0.79, respectively.
One item of cultural awareness and two items of cultural encounters were eliminated because of CITC<0.4 (Table 1). A total of 21 items entered the exploratory EFA. KMO was equal to 0.906, and Bartlett’s test was also significant at an acceptable level (P<0.001); therefore, the achieved data were appropriate for EFA. Five factors were extracted according to eigenvalues >1 and factors loads of ≥0.4. Overall five factors of cultural skill, cultural awareness, cultural desire, cultural encounters, and cultural behavior described 62.44 % of the assumed model (Table 2).
Cronbach’s α coefficient of each construct was as follows: cultural skill (α=0.85); cultural awareness (α=0.80); cultural desire (α=0.80); cultural encounters (α=0.81), and cultural behavior (α=0.70) (Table 2). The scree plot of the structures studied among the participants is presented in Figure 1. The Mean±SD score of cultural competency was 65.94±10.30, ranging from 21 to 105; the study participants achieved 62.8% of the maximum obtainable score for cultural competency.
4. Discussion
The present study determined the psychometric properties of CCS among Iranian healthcare providers. The attained results indicated the investigated CCS is adequately reliable and valid for the measurement of CC among Iranian healthcare providers. Some studies have stated developing accurate items that measure specific construct without error is difficult, because of individual beliefs without affecting their other beliefs it does not happen [30, 31]. For example, in this study, the cultural awareness of study participants may have affected their other beliefs, such as cultural desire and cultural encounters.
Our findings indicated that the constructs of CCS greater than 0.70 were interactively inconsistent; these results suggest CCS is an acceptable instrument for measuring CC among Iranian healthcare providers. Liu et al. studied 533 registered nurses in Macao to evaluate the reliability and validity of the competency inventory. They concluded internal consistency and Cronbach’s α coefficient of scale were 0.908 and 0.718 to 0.903 for subscales [16]. Furthermore, Campinha-Bacote introduced a questionnaire of CC in the delivery of healthcare; it is one of the most widely used scales of CC among healthcare providers. It explores cultural awareness, cultural knowledge, cultural skill, cultural encounters, and cultural desire [17].
Our results indicated the cultural competency constructs described 62.44% of the assumed model. Moreover, cultural skill, cultural desire, and cultural awareness were the stronger predictors of the assumed model, respectively. In this regard, Suurmond emphasized on the promotion of cultural awareness in healthcare providers [32]. Therefore, it seems that improving cultural awareness is an appropriate strategy for promoting CC among healthcare providers.
Another finding of our study indicated the study participants achieved 62.8% of the maximum obtainable score for CC. In this regard, Kardong-Edgren et al. [33] and Riley et al. [34] reported that CC status among healthcare providers was at a medium level. This result is consistent with our study. These data can alarm health policymakers and highlight the necessity to the development of CC promotion programs among healthcare providers.
The present study is important according to the limitations of the questionnaire on the assessment of cultural competence among Iranian healthcare providers. However, our research had some limitations; e.g. gathering information based on self-report, which always faces the risk of recall bias and provide incorrect information by respondents.
5. Conclusion
CCS is a valid and reliable tool for measuring CC among Iranian healthcare providers. CCS can be applied for behavior change studies among Iranian healthcare providers with the aim of CC promotion.
Ethical Considerations
Compliance with ethical guidelines
The Research Ethics Committee at Deputy of Research of the Kermanshah University of Medical Sciences (KUMS.REC.1394.448) had approved the study protocol and had monitored the research process. Furthermore, the study participants were provided with the participant information statement and signed the written informed consent forms. Their personal information was kept confidential.
Funding
This article is a part of a research project supported by Kermanshah University of Medical Sciences.
Authors' contributions
Developing the original idea, and data analysis: Mehdi Mirzaei-Alavijeh and Farzad Jalilian; Study design: Behzad Karami Matin and Farid Najafi. Approving the final manuscript: All author’s authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We would like to thank the deputy of research of Kermanshah University of Medical Sciences for its financial support.
References
Vincens N, Emmelin M, Stafström M. Social capital, income inequality and the social gradient in self-rated health in Latin America: A fixed effects analysis. Social Science & Medicine. 2018; 196:115-22. [DOI:10.1016/j.socscimed.2017.11.025] [PMID]
Thresia CU. Health inequalities in South Asia at the launch of sustainable development goals: Exclusions in health in Kerala, India need political interventions. International Journal of Health Services. 2018; 48(1):57-80. [DOI:10.1177/0020731417738222] [PMID]
Whitehead M. The concepts and principles of equity and health. Health Promotion International. 1991; 6(3):217-28 [DOI:10.1093/heapro/6.3.217]
Miguel A, Luquis RR. Cultural competence in health education and health promotion. Hoboken: John Wiley & Sons; 2013.
Chen J, Vargas-Bustamante A, Mortensen K, Ortega AN. Racial and ethnic disparities in health care access and utilization under the affordable care act. Medical Care. 2016; 54(2):140. [DOI:10.1097/MLR.0000000000000467] [PMID] [PMCID]
Flores G, Lin H. Trends in racial/ ethnic disparities in medical and oral health, access to care, and use of services in US children: Has anything changed over the years? International Journal for Equity in Health. 2013; 12:10. [DOI:10.1186/1475-9276-12-10] [PMID] [PMCID]
Brach C, Fraserirector I. Can cultural competency reduce racial and ethnic health disparities? A review and conceptual model. Medical Care Research and Review. 2000; 57(1-suppl):181-217. [DOI:10.1177/1077558700057001S09] [PMID] [PMCID]
Lin CJ, Lee CK, Huang MC. Cultural competence of health care providers: A systematic review of assessment instruments. Journal of Nursing Research. 2017; 25(3):174-86. [DOI:10.1097/JNR.0000000000000153]
McCalman J, Jongen C, Bainbridge R. Organisational systems’ approaches to improving cultural competence in healthcare: A systematic scoping review of the literature. International Journal for Equity in Health. 2017; 16:78. [DOI:10.1186/s12939-017-0571-5] [PMID] [PMCID]
Young S, Guo KL. Cultural diversity training: The necessity of cultural competence for health care providers and in nursing practice. The Health Care Manager. 2016; 35(2):94-102 [DOI:10.1097/HCM.0000000000000100] [PMID]
Sequist TD, Fitzmaurice GM, Marshall R, Shaykevich S, Marston A, Safran DG, et al. Cultural competency training and performance reports to improve diabetes care for black patients: A cluster randomized, controlled trial. Annals of Internal Medicine. 2010; 152(1):40-6. [DOI:10.7326/0003-4819-152-1-201001050-00009] [PMID]
Lie DA, Lee-Rey E, Gomez A, Bereknyei S, Braddock CH. Does cultural competency training of health professionals improve patient outcomes? A systematic review and proposed algorithm for future research. Journal of General Internal Medicine. 2011; 26(3):317-25. [DOI:10.1007/s11606-010-1529-0] [PMID] [PMCID]
Garneau AB, Pepin J. Cultural competence: A constructivist definition. Journal of Transcultural Nursing. 2015; 26(1):9-15 [DOI:10.1177/1043659614541294] [PMID]
Shen Z. Cultural competence models and cultural competence assessment instruments in nursing: A literature review. Journal of Transcultural Nursing. 2015; 26(3):308-21 [DOI:10.1177/1043659614524790] [PMID]
Davis Jr PC, Rankin LL. Guidelines for making existing health education programs more culturally appropriate. American Journal of Health Education. 2006; 37(4):250-2. [DOI:10.1080/19325037.2006.10598912]
Liu M, Yin L, Ma E, Lo S, Zeng L. Competency inventory for registered nurses in Macao: Instrument validation. Journal of Advanced Nursing. 2009; 65(4): 893-900. [DOI:10.1111/j.1365-2648.2008.04936.x] [PMID]
Campinha-Bacote J. The process of cultural competence in the delivery of health care services: A model of care. Journal of Transcultural Nursing. 2002; 13(3):181-4. [DOI:10.1177/10459602013003003] [PMID]
Truong M, Paradies Y, Priest N. Interventions to improve cultural competency in healthcare: A systematic review of reviews. BMC Health Services Research. 2014; 14:99. [DOI:10.1186/1472-6963-14-99] [PMID] [PMCID]
Matsumoto D, Hwang HC. Assessing cross-cultural competence: A review of available tests. Journal of Cross-Cultural Psychology. 2013; 44(6):849-73. [DOI:10.1177/0022022113492891]
Davis TS. Mapping patterns of perceptions: A community-based approach to cultural competence assessment. Research on Social Work Practice. 2007; 17(3):358-79. [DOI:10.1177/1049731506295103]
Alavijeh MM, Matin BK, Jalilian F, Hamzeh B, Haghighi M, Ahmadpanah M, et al. Relapse preventative intervention among Iranian addicts based on theory of planned behavior results. Research Journal of Applied Sciences. 2016; 11(4):138-43. [DOI:10.3923/rjasci.2016.138.143]
Hosseini SN, Alavijeh MM, Matin BK, Hamzeh B, Ashtarian H, Jalilian F. Locus of control or self-esteem; Which one is the best predictor of academic achievement in Iranian college students. Iranian Journal of Psychiatry and Behavioral Sciences. 2016; 10(1):e2602. [DOI:10.17795/ijpbs-2602] [PMID] [PMCID]
Mirzaei-Alavijeh M, Zolghadr R, Fattahi M, Jalilian F. Demographic characteristics associated with vulnerability of oral diseases among primary school students in Southern of Iran. International Journal of Pediatrics. 2017; 5(12):6555-62. [DOI:10.22038/IJP.2017.27195.2339]
Jalilian F, Moazami P, Mirzaei-Alavijeh M, Moazami AM, Jalili C. Sensation seeking and the intention to cheating among college students: An application of the theory of planned behavior. Research Journal of Applied Sciences. 2016; 11(8):645-9. [DOI:10.3923/rjasci.2016.645.649]
Mirzaei-Alavijeh M, Ahmadi-Jouybari T, Vaezi M, Jalilian F. Prevalence, cognitive and socio-demographic determinants of prostate cancer screening. Asian Pacific Journal of Cancer Prevention. 2018; 19(4):1041-6. [PMID] [PMCID]
Mirzaei-Alavijeh M, Ghorbani P, Jalilian F. Socio-cognitive determinants of the mammography screening uptake among Iranian women. Asian Pacific Journal of Cancer Prevention. 2018; 19(5):1351-5. [PMID] [PMCID]
Samii AW. The nation and its minorities: Ethnicity, unity, and state policy in Iran. Comparative Studies of South Asia, Africa and the Middle East. 2000; 20(1):128-37. [DOI:10.1215/1089201X-20-1-2-128]
Knapp TR, Brown JK. Ten measurement commandments that often broken. Research in Nursing & Health. 1995; 18(5):465-9 . [DOI:10.1002/nur.4770180511]
Thompson B. Exploratory and confirmatory factor analysis: Understanding concepts and applications. American Psychological Association; 2004. [DOI:10.1037/10694-000]
Jalilian F, Mirzaei-Alavijeh M, Ahmadpanah M, Matin BK, Ataee M, Eslami AA, et al. Psychometrics of the instrument measuring beliefs related to drug abuse among iranian college students. Journal of Health Management. 2017; 19(3):377-86. [DOI:10.1177/0972063416651595]
Mirzaei-Alavijeh M, Vaezi M, Jalilian F. [Psychometric evaluation of a theory based colorectal cancer screening questionnaire with uptake of fecal occult blood test (Persian)]. Govaresh. 2018; 23(2):77-83.
Suurmond J, Seeleman C, Rupp I, Goosen S, Stronks K. Cultural competence among nurse practitioners working with asylum seekers. Nurse Education Today. 2010; 30(8):821-6 [DOI:10.1016/j.nedt.2010.03.006] [PMID]
Kardong-Edgren S, Bond ML, Schlosser S, Cason C, Jones ME, Warr R, et al. Cultural attitudes, knowledge, and skills of nursing faculty toward patients from four diverse cultures. Journal of Professional Nursing. 2005; 21(3):175-82. [DOI:10.1016/j.profnurs.2005.04.001] [PMID]
Riley D, Smyer T, York N. Cultural competence of practicing nurses entering an RN-BSN program. Nursing Education Perspectives. 2012; 33(6):381-5. [DOI:10.5480/1536-5026-33.6.381] [PMID]
The present study determined the psychometric properties of CCS among Iranian healthcare providers. The attained results indicated the investigated CCS is adequately reliable and valid for the measurement of CC among Iranian healthcare providers. Some studies have stated developing accurate items that measure specific construct without error is difficult, because of individual beliefs without affecting their other beliefs it does not happen [30, 31]. For example, in this study, the cultural awareness of study participants may have affected their other beliefs, such as cultural desire and cultural encounters.
Our findings indicated that the constructs of CCS greater than 0.70 were interactively inconsistent; these results suggest CCS is an acceptable instrument for measuring CC among Iranian healthcare providers. Liu et al. studied 533 registered nurses in Macao to evaluate the reliability and validity of the competency inventory. They concluded internal consistency and Cronbach’s α coefficient of scale were 0.908 and 0.718 to 0.903 for subscales [16]. Furthermore, Campinha-Bacote introduced a questionnaire of CC in the delivery of healthcare; it is one of the most widely used scales of CC among healthcare providers. It explores cultural awareness, cultural knowledge, cultural skill, cultural encounters, and cultural desire [17].
Our results indicated the cultural competency constructs described 62.44% of the assumed model. Moreover, cultural skill, cultural desire, and cultural awareness were the stronger predictors of the assumed model, respectively. In this regard, Suurmond emphasized on the promotion of cultural awareness in healthcare providers [32]. Therefore, it seems that improving cultural awareness is an appropriate strategy for promoting CC among healthcare providers.
Another finding of our study indicated the study participants achieved 62.8% of the maximum obtainable score for CC. In this regard, Kardong-Edgren et al. [33] and Riley et al. [34] reported that CC status among healthcare providers was at a medium level. This result is consistent with our study. These data can alarm health policymakers and highlight the necessity to the development of CC promotion programs among healthcare providers.
The present study is important according to the limitations of the questionnaire on the assessment of cultural competence among Iranian healthcare providers. However, our research had some limitations; e.g. gathering information based on self-report, which always faces the risk of recall bias and provide incorrect information by respondents.
5. Conclusion
CCS is a valid and reliable tool for measuring CC among Iranian healthcare providers. CCS can be applied for behavior change studies among Iranian healthcare providers with the aim of CC promotion.
Ethical Considerations
Compliance with ethical guidelines
The Research Ethics Committee at Deputy of Research of the Kermanshah University of Medical Sciences (KUMS.REC.1394.448) had approved the study protocol and had monitored the research process. Furthermore, the study participants were provided with the participant information statement and signed the written informed consent forms. Their personal information was kept confidential.
Funding
This article is a part of a research project supported by Kermanshah University of Medical Sciences.
Authors' contributions
Developing the original idea, and data analysis: Mehdi Mirzaei-Alavijeh and Farzad Jalilian; Study design: Behzad Karami Matin and Farid Najafi. Approving the final manuscript: All author’s authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We would like to thank the deputy of research of Kermanshah University of Medical Sciences for its financial support.
References
Vincens N, Emmelin M, Stafström M. Social capital, income inequality and the social gradient in self-rated health in Latin America: A fixed effects analysis. Social Science & Medicine. 2018; 196:115-22. [DOI:10.1016/j.socscimed.2017.11.025] [PMID]
Thresia CU. Health inequalities in South Asia at the launch of sustainable development goals: Exclusions in health in Kerala, India need political interventions. International Journal of Health Services. 2018; 48(1):57-80. [DOI:10.1177/0020731417738222] [PMID]
Whitehead M. The concepts and principles of equity and health. Health Promotion International. 1991; 6(3):217-28 [DOI:10.1093/heapro/6.3.217]
Miguel A, Luquis RR. Cultural competence in health education and health promotion. Hoboken: John Wiley & Sons; 2013.
Chen J, Vargas-Bustamante A, Mortensen K, Ortega AN. Racial and ethnic disparities in health care access and utilization under the affordable care act. Medical Care. 2016; 54(2):140. [DOI:10.1097/MLR.0000000000000467] [PMID] [PMCID]
Flores G, Lin H. Trends in racial/ ethnic disparities in medical and oral health, access to care, and use of services in US children: Has anything changed over the years? International Journal for Equity in Health. 2013; 12:10. [DOI:10.1186/1475-9276-12-10] [PMID] [PMCID]
Brach C, Fraserirector I. Can cultural competency reduce racial and ethnic health disparities? A review and conceptual model. Medical Care Research and Review. 2000; 57(1-suppl):181-217. [DOI:10.1177/1077558700057001S09] [PMID] [PMCID]
Lin CJ, Lee CK, Huang MC. Cultural competence of health care providers: A systematic review of assessment instruments. Journal of Nursing Research. 2017; 25(3):174-86. [DOI:10.1097/JNR.0000000000000153]
McCalman J, Jongen C, Bainbridge R. Organisational systems’ approaches to improving cultural competence in healthcare: A systematic scoping review of the literature. International Journal for Equity in Health. 2017; 16:78. [DOI:10.1186/s12939-017-0571-5] [PMID] [PMCID]
Young S, Guo KL. Cultural diversity training: The necessity of cultural competence for health care providers and in nursing practice. The Health Care Manager. 2016; 35(2):94-102 [DOI:10.1097/HCM.0000000000000100] [PMID]
Sequist TD, Fitzmaurice GM, Marshall R, Shaykevich S, Marston A, Safran DG, et al. Cultural competency training and performance reports to improve diabetes care for black patients: A cluster randomized, controlled trial. Annals of Internal Medicine. 2010; 152(1):40-6. [DOI:10.7326/0003-4819-152-1-201001050-00009] [PMID]
Lie DA, Lee-Rey E, Gomez A, Bereknyei S, Braddock CH. Does cultural competency training of health professionals improve patient outcomes? A systematic review and proposed algorithm for future research. Journal of General Internal Medicine. 2011; 26(3):317-25. [DOI:10.1007/s11606-010-1529-0] [PMID] [PMCID]
Garneau AB, Pepin J. Cultural competence: A constructivist definition. Journal of Transcultural Nursing. 2015; 26(1):9-15 [DOI:10.1177/1043659614541294] [PMID]
Shen Z. Cultural competence models and cultural competence assessment instruments in nursing: A literature review. Journal of Transcultural Nursing. 2015; 26(3):308-21 [DOI:10.1177/1043659614524790] [PMID]
Davis Jr PC, Rankin LL. Guidelines for making existing health education programs more culturally appropriate. American Journal of Health Education. 2006; 37(4):250-2. [DOI:10.1080/19325037.2006.10598912]
Liu M, Yin L, Ma E, Lo S, Zeng L. Competency inventory for registered nurses in Macao: Instrument validation. Journal of Advanced Nursing. 2009; 65(4): 893-900. [DOI:10.1111/j.1365-2648.2008.04936.x] [PMID]
Campinha-Bacote J. The process of cultural competence in the delivery of health care services: A model of care. Journal of Transcultural Nursing. 2002; 13(3):181-4. [DOI:10.1177/10459602013003003] [PMID]
Truong M, Paradies Y, Priest N. Interventions to improve cultural competency in healthcare: A systematic review of reviews. BMC Health Services Research. 2014; 14:99. [DOI:10.1186/1472-6963-14-99] [PMID] [PMCID]
Matsumoto D, Hwang HC. Assessing cross-cultural competence: A review of available tests. Journal of Cross-Cultural Psychology. 2013; 44(6):849-73. [DOI:10.1177/0022022113492891]
Davis TS. Mapping patterns of perceptions: A community-based approach to cultural competence assessment. Research on Social Work Practice. 2007; 17(3):358-79. [DOI:10.1177/1049731506295103]
Alavijeh MM, Matin BK, Jalilian F, Hamzeh B, Haghighi M, Ahmadpanah M, et al. Relapse preventative intervention among Iranian addicts based on theory of planned behavior results. Research Journal of Applied Sciences. 2016; 11(4):138-43. [DOI:10.3923/rjasci.2016.138.143]
Hosseini SN, Alavijeh MM, Matin BK, Hamzeh B, Ashtarian H, Jalilian F. Locus of control or self-esteem; Which one is the best predictor of academic achievement in Iranian college students. Iranian Journal of Psychiatry and Behavioral Sciences. 2016; 10(1):e2602. [DOI:10.17795/ijpbs-2602] [PMID] [PMCID]
Mirzaei-Alavijeh M, Zolghadr R, Fattahi M, Jalilian F. Demographic characteristics associated with vulnerability of oral diseases among primary school students in Southern of Iran. International Journal of Pediatrics. 2017; 5(12):6555-62. [DOI:10.22038/IJP.2017.27195.2339]
Jalilian F, Moazami P, Mirzaei-Alavijeh M, Moazami AM, Jalili C. Sensation seeking and the intention to cheating among college students: An application of the theory of planned behavior. Research Journal of Applied Sciences. 2016; 11(8):645-9. [DOI:10.3923/rjasci.2016.645.649]
Mirzaei-Alavijeh M, Ahmadi-Jouybari T, Vaezi M, Jalilian F. Prevalence, cognitive and socio-demographic determinants of prostate cancer screening. Asian Pacific Journal of Cancer Prevention. 2018; 19(4):1041-6. [PMID] [PMCID]
Mirzaei-Alavijeh M, Ghorbani P, Jalilian F. Socio-cognitive determinants of the mammography screening uptake among Iranian women. Asian Pacific Journal of Cancer Prevention. 2018; 19(5):1351-5. [PMID] [PMCID]
Samii AW. The nation and its minorities: Ethnicity, unity, and state policy in Iran. Comparative Studies of South Asia, Africa and the Middle East. 2000; 20(1):128-37. [DOI:10.1215/1089201X-20-1-2-128]
Knapp TR, Brown JK. Ten measurement commandments that often broken. Research in Nursing & Health. 1995; 18(5):465-9 . [DOI:10.1002/nur.4770180511]
Thompson B. Exploratory and confirmatory factor analysis: Understanding concepts and applications. American Psychological Association; 2004. [DOI:10.1037/10694-000]
Jalilian F, Mirzaei-Alavijeh M, Ahmadpanah M, Matin BK, Ataee M, Eslami AA, et al. Psychometrics of the instrument measuring beliefs related to drug abuse among iranian college students. Journal of Health Management. 2017; 19(3):377-86. [DOI:10.1177/0972063416651595]
Mirzaei-Alavijeh M, Vaezi M, Jalilian F. [Psychometric evaluation of a theory based colorectal cancer screening questionnaire with uptake of fecal occult blood test (Persian)]. Govaresh. 2018; 23(2):77-83.
Suurmond J, Seeleman C, Rupp I, Goosen S, Stronks K. Cultural competence among nurse practitioners working with asylum seekers. Nurse Education Today. 2010; 30(8):821-6 [DOI:10.1016/j.nedt.2010.03.006] [PMID]
Kardong-Edgren S, Bond ML, Schlosser S, Cason C, Jones ME, Warr R, et al. Cultural attitudes, knowledge, and skills of nursing faculty toward patients from four diverse cultures. Journal of Professional Nursing. 2005; 21(3):175-82. [DOI:10.1016/j.profnurs.2005.04.001] [PMID]
Riley D, Smyer T, York N. Cultural competence of practicing nurses entering an RN-BSN program. Nursing Education Perspectives. 2012; 33(6):381-5. [DOI:10.5480/1536-5026-33.6.381] [PMID]
Article Type: Research Article |
Subject:
Psychiatry
Received: 2017/05/22 | Accepted: 2017/08/17 | Published: 2017/11/1
Received: 2017/05/22 | Accepted: 2017/08/17 | Published: 2017/11/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Hamadan University of Medical Sciences.
Published by UMSHA Press
Journal Tel: +989025126654
Publisher Tel: +985138419434
Website: http://ajnpp.umsha.ac.ir
Email: avicennajnpp[at]gmail.com
