

Volume 6, Issue 1 (Februrary 2019)
Avicenna J Neuro Psycho Physiology 2019, 6(1): 19-26 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rostami Nezhad S, Arefi M, Khademi A. The Effectiveness of Dialectical Behavior Therapy on the Addiction-Prone Male Junior High School Students. Avicenna J Neuro Psycho Physiology 2019; 6 (1) :19-26
URL: http://ajnpp.umsha.ac.ir/article-1-149-en.html
URL: http://ajnpp.umsha.ac.ir/article-1-149-en.html



1- Department of Psychology, Urmia Branch, Islamic Azad University, Urmia, Iran.
2- Department of Psychology, Urmia Branch, Islamic Azad University, Urmia, Iran. , m.arefi@iaurmia.ac.ir
2- Department of Psychology, Urmia Branch, Islamic Azad University, Urmia, Iran. , m.arefi@iaurmia.ac.ir
Full-Text [PDF 642 kb]
(1143 Downloads)
| Abstract (HTML) (2667 Views)
Full-Text: (644 Views)
1. Introduction
Addiction is a psychosocial phenomenon, whose etiology lies in family relationships, social relationships, critical and cultural conditions, and, ultimately, the psychological characteristics of the addicted person [1]. The tendency to narcotics is one of the serious problems of human society. The theory of addiction (addiction preparation) suggests that some people are susceptible to addiction and become addicted if they are exposed to drugs; but, if a person does not have the ability to become addicted [2], predisposing factors (mental illness, behavioral incompatibilities, and personality problems) can exacerbate the possibility of addiction [3]. Increasing drug and psychotropic use are a growing concern for all societies over the last century [4]. According to Iran Drug Control Headquarters, 1% of the students consume drugs, which, of course, does not mean that they are addicted and include entertaining consumption. Also, 60% of adult consumers have begun drug use since they were students. In Iran, so far, 12.12% of male students have consumed alcohol, while 2% of them have used drugs (unauthorized) [5].
Meanwhile, Dialectical Behavior Therapy (DBT) is one of the most effective approaches to control drug use. The main body of this method is to educate and focus on the learning, application, and deployment of specific adaptive skills, whose ultimate goal is helping the patient to break in and overcome the difficult situations of defective cycles and conflicts [6]. DBT is based on the continuous evaluation and data collection related to current behaviors, explicit definition of therapeutic goals, and the relationship between therapist and patient collaboration. Many of the components of DBT, such as problem-solving, exposure, skill training, conditional management, and cognitive change have long been used in cognitive-behavioral therapy.
This treatment is effective for patients seeking to control emotional disturbances [7]. DBT was developed to reduce self-harming behaviors in patients with a borderline personality disorder that was faced with extreme emotional challenges [8]. Over the past few years, it has been used for a range of mental health challenges, including emotional and emotional disturbances, self-harm behaviors, suicide, addictive behaviors, depression, and anxiety [9]. In standard DBT, the main goals of addiction treatment include the reduction of the temptation to consume, the control of severe behaviors (adjusting emotions and endurance distress), the reduction of life-threatening behaviors (drug use and suicide), the increase of adaptive behaviors and learning skills, including mindfulness and interpersonal efficiency [10]. Regarding the decreased age of addiction tendency and increasing addiction among students because of the lack of individual skills in dealing with rapid changes in adolescence, as a threat to health and mental health, students are more likely to become addicted [11]. More than 30,000 of the Iranian students are addicted. The drug use in the age group of 15-19 years old was 13.56% of the total population of drug addicts throughout the country, requiring the use of educational and therapeutic services [12]. The use of newer therapeutic approaches such as DBT, as the third wave of behavioral therapy that was successful in treating patients with borderline personality disorder, seems to be successful. The researcher intends to examine the effectiveness of these therapies on adolescents, who are more likely to be addicted. Therefore, this study aimed at investigating the effectiveness of DBT on the addiction-prone male junior high school students.
2. Materials and Methods
The present quasi-experimental study used a pretest-posttest design with a control group. The statistical population of this study includes all 10th-grade male students in Tonekabon, Iran, in the academic year 2016-2017. The number of samples was determined by the Cochran formula and selected by random cluster sampling. They were assigned to the experimental and control groups.
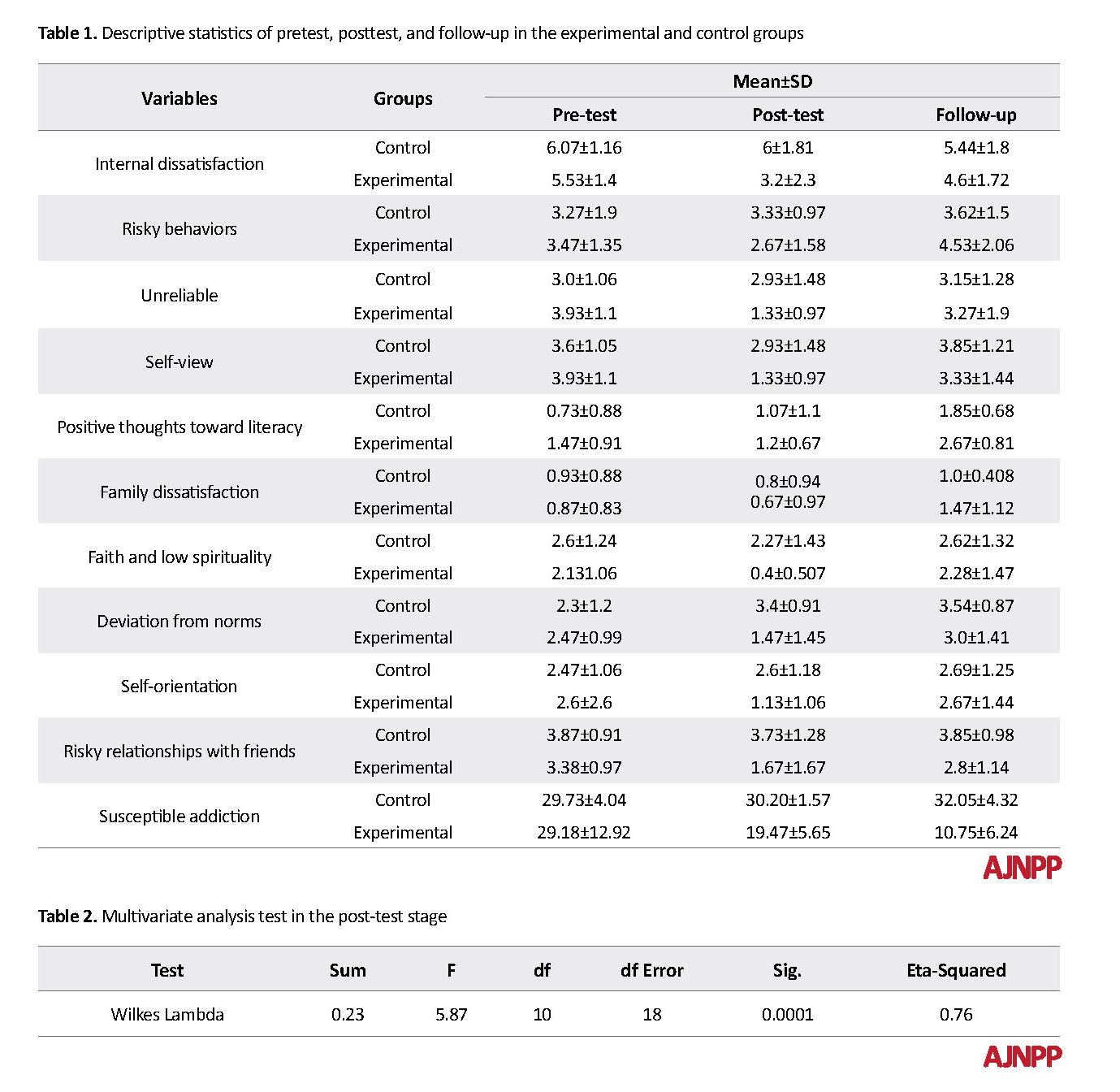
In this research, the samples were selected from the 10th-grade students and multistage random cluster sampling was used. Five schools were randomly selected from high schools in Tonekabon. To select the required statistical sample, firstly, in each of the designated schools, the Addiction-Prone Questionnaire in Iranian adolescents was distributed among all 10th-grade students. After completing the questionnaire, several students scored high; among them, a few were randomly selected and assigned to the experimental group under the group psychotherapy of DBT. A control group was selected, and no therapeutic consideration was made on them. The implementation of this research began in early May of 2015, and the intervention lasted from November to late December 2016 and generally consisted of pretest, posttest, and follow-up stages (Table 1).
In the present study, firstly, by referring to the Education Department, the list of high schools in Tonekabon was provided to the researcher. Then, 5 schools were selected through random cluster sampling, and the addiction-prone scale for Iranian adolescents was distributed among the students. Before submitting the test, a brief explanation was given on why this test was conducted, and students were asked to answer the questions. Moreover, their response would not have any effect on their relationship with school agents and their discipline mark, and their honest cooperation would help them take a step forward in advancing knowledge and science. Then, the test instructions were read to the students. If there was a problem in understanding each question, the researcher would clearly explain it. Of the students, who scored above 25 (low talent), 60 were randomly assigned to the experimental and control groups (each group consisted of 30 students). Since it was not possible to gather the students during the summer, the intervention was postponed to the new academic year in October 2016.
At this stage, 60 students, who scored high in the adolescent addiction-prone scale, were randomly selected and divided into two groups. The experimental group was given interventional DBT and the control group experienced no treatment. Each session lasted 60 minutes once a week in one of the schools; the sessions were over in late December.
Addiction-Prone Questionnaire in Iranian Adolescents
Zeinali, Vahdat, and Hamednia in 2007 designed this questionnaire to measure being prone to addiction. This questionnaire measures the psychosocial factors involved in drug abuse with a developmental perspective, and it is used by the general population and consistent with the culture of Iranian people. The questionnaire consists of 50 items that are scored on a 2-tier scale (0=yes and 1=no). The validity of the questionnaire was 66% with the risk profile of drug use [13]. The validity and reliability of this questionnaire were 0.73 and 0.78, respectively.
The two first sessions of distress tolerance skills were dedicated to necessary skills of tolerating distress and distraction (fundamental acceptance, distraction from self-damaging behaviors, joyful activities, concentration on work or other issues, distraction, distraction by leaving the situation, distraction by assigning daily works, distraction by counting, setting distraction programs, self-calming, and codifying resting design). In the next two sessions, the advanced skills were focused (visualizing a safe environment, discovering values, detecting superpowers, living at the moment, using self-motivating defensive thoughts, essential acceptance, self-confirming utterance, and setting defensive approaches). The fifth and sixth sessions focused on the necessary skills of emotional discipline, including detecting emotions, how the emotions act, removing obstacles of healthy emotions, reducing damages caused by distressing emotions, self-monitoring, cutting cognitive vulnerability, and improving positive emotions. Finally, the last two sessions were dedicated to the advanced skills of emotional regulation, including intentional concentration on emotions instead of judging them, dealing with emotions, acting despite intense emotions, and problem-solving. The data were analyzed by SPSS v. 22, using the analysis of repeated measures in pretest, posttest, and follow-up stages with a significance level of P<0.05.
3. Results
The Mean±SD of the students was 13.6±4.4 and 13.1±4.0 in the experimental group and the control group, respectively. According to the M box test, F equals 0.996 and the significance level of the test equals 48.33; so, the null hypothesis based on matrix homogeneity and variance of the covariance of DBT and control is confirmed (Table 2). The interactive effects (group and sub-scales of susceptible addiction pretest) in the posttest stage have higher levels than the 5% error (P>0.05); so, the assumption of homogeneity of regression slopes is also established. It is possible to use a repeated measure analysis (Table 3). Significant levels for Leven’s test in each subscale are more than 5% error; so, the assumption of homogeneity of error variances is acceptable for the control group and the experimental group.
Addiction is a psychosocial phenomenon, whose etiology lies in family relationships, social relationships, critical and cultural conditions, and, ultimately, the psychological characteristics of the addicted person [1]. The tendency to narcotics is one of the serious problems of human society. The theory of addiction (addiction preparation) suggests that some people are susceptible to addiction and become addicted if they are exposed to drugs; but, if a person does not have the ability to become addicted [2], predisposing factors (mental illness, behavioral incompatibilities, and personality problems) can exacerbate the possibility of addiction [3]. Increasing drug and psychotropic use are a growing concern for all societies over the last century [4]. According to Iran Drug Control Headquarters, 1% of the students consume drugs, which, of course, does not mean that they are addicted and include entertaining consumption. Also, 60% of adult consumers have begun drug use since they were students. In Iran, so far, 12.12% of male students have consumed alcohol, while 2% of them have used drugs (unauthorized) [5].
Meanwhile, Dialectical Behavior Therapy (DBT) is one of the most effective approaches to control drug use. The main body of this method is to educate and focus on the learning, application, and deployment of specific adaptive skills, whose ultimate goal is helping the patient to break in and overcome the difficult situations of defective cycles and conflicts [6]. DBT is based on the continuous evaluation and data collection related to current behaviors, explicit definition of therapeutic goals, and the relationship between therapist and patient collaboration. Many of the components of DBT, such as problem-solving, exposure, skill training, conditional management, and cognitive change have long been used in cognitive-behavioral therapy.
This treatment is effective for patients seeking to control emotional disturbances [7]. DBT was developed to reduce self-harming behaviors in patients with a borderline personality disorder that was faced with extreme emotional challenges [8]. Over the past few years, it has been used for a range of mental health challenges, including emotional and emotional disturbances, self-harm behaviors, suicide, addictive behaviors, depression, and anxiety [9]. In standard DBT, the main goals of addiction treatment include the reduction of the temptation to consume, the control of severe behaviors (adjusting emotions and endurance distress), the reduction of life-threatening behaviors (drug use and suicide), the increase of adaptive behaviors and learning skills, including mindfulness and interpersonal efficiency [10]. Regarding the decreased age of addiction tendency and increasing addiction among students because of the lack of individual skills in dealing with rapid changes in adolescence, as a threat to health and mental health, students are more likely to become addicted [11]. More than 30,000 of the Iranian students are addicted. The drug use in the age group of 15-19 years old was 13.56% of the total population of drug addicts throughout the country, requiring the use of educational and therapeutic services [12]. The use of newer therapeutic approaches such as DBT, as the third wave of behavioral therapy that was successful in treating patients with borderline personality disorder, seems to be successful. The researcher intends to examine the effectiveness of these therapies on adolescents, who are more likely to be addicted. Therefore, this study aimed at investigating the effectiveness of DBT on the addiction-prone male junior high school students.
2. Materials and Methods
The present quasi-experimental study used a pretest-posttest design with a control group. The statistical population of this study includes all 10th-grade male students in Tonekabon, Iran, in the academic year 2016-2017. The number of samples was determined by the Cochran formula and selected by random cluster sampling. They were assigned to the experimental and control groups.
In this research, the samples were selected from the 10th-grade students and multistage random cluster sampling was used. Five schools were randomly selected from high schools in Tonekabon. To select the required statistical sample, firstly, in each of the designated schools, the Addiction-Prone Questionnaire in Iranian adolescents was distributed among all 10th-grade students. After completing the questionnaire, several students scored high; among them, a few were randomly selected and assigned to the experimental group under the group psychotherapy of DBT. A control group was selected, and no therapeutic consideration was made on them. The implementation of this research began in early May of 2015, and the intervention lasted from November to late December 2016 and generally consisted of pretest, posttest, and follow-up stages (Table 1).
In the present study, firstly, by referring to the Education Department, the list of high schools in Tonekabon was provided to the researcher. Then, 5 schools were selected through random cluster sampling, and the addiction-prone scale for Iranian adolescents was distributed among the students. Before submitting the test, a brief explanation was given on why this test was conducted, and students were asked to answer the questions. Moreover, their response would not have any effect on their relationship with school agents and their discipline mark, and their honest cooperation would help them take a step forward in advancing knowledge and science. Then, the test instructions were read to the students. If there was a problem in understanding each question, the researcher would clearly explain it. Of the students, who scored above 25 (low talent), 60 were randomly assigned to the experimental and control groups (each group consisted of 30 students). Since it was not possible to gather the students during the summer, the intervention was postponed to the new academic year in October 2016.
At this stage, 60 students, who scored high in the adolescent addiction-prone scale, were randomly selected and divided into two groups. The experimental group was given interventional DBT and the control group experienced no treatment. Each session lasted 60 minutes once a week in one of the schools; the sessions were over in late December.
Addiction-Prone Questionnaire in Iranian Adolescents
Zeinali, Vahdat, and Hamednia in 2007 designed this questionnaire to measure being prone to addiction. This questionnaire measures the psychosocial factors involved in drug abuse with a developmental perspective, and it is used by the general population and consistent with the culture of Iranian people. The questionnaire consists of 50 items that are scored on a 2-tier scale (0=yes and 1=no). The validity of the questionnaire was 66% with the risk profile of drug use [13]. The validity and reliability of this questionnaire were 0.73 and 0.78, respectively.
The two first sessions of distress tolerance skills were dedicated to necessary skills of tolerating distress and distraction (fundamental acceptance, distraction from self-damaging behaviors, joyful activities, concentration on work or other issues, distraction, distraction by leaving the situation, distraction by assigning daily works, distraction by counting, setting distraction programs, self-calming, and codifying resting design). In the next two sessions, the advanced skills were focused (visualizing a safe environment, discovering values, detecting superpowers, living at the moment, using self-motivating defensive thoughts, essential acceptance, self-confirming utterance, and setting defensive approaches). The fifth and sixth sessions focused on the necessary skills of emotional discipline, including detecting emotions, how the emotions act, removing obstacles of healthy emotions, reducing damages caused by distressing emotions, self-monitoring, cutting cognitive vulnerability, and improving positive emotions. Finally, the last two sessions were dedicated to the advanced skills of emotional regulation, including intentional concentration on emotions instead of judging them, dealing with emotions, acting despite intense emotions, and problem-solving. The data were analyzed by SPSS v. 22, using the analysis of repeated measures in pretest, posttest, and follow-up stages with a significance level of P<0.05.
3. Results
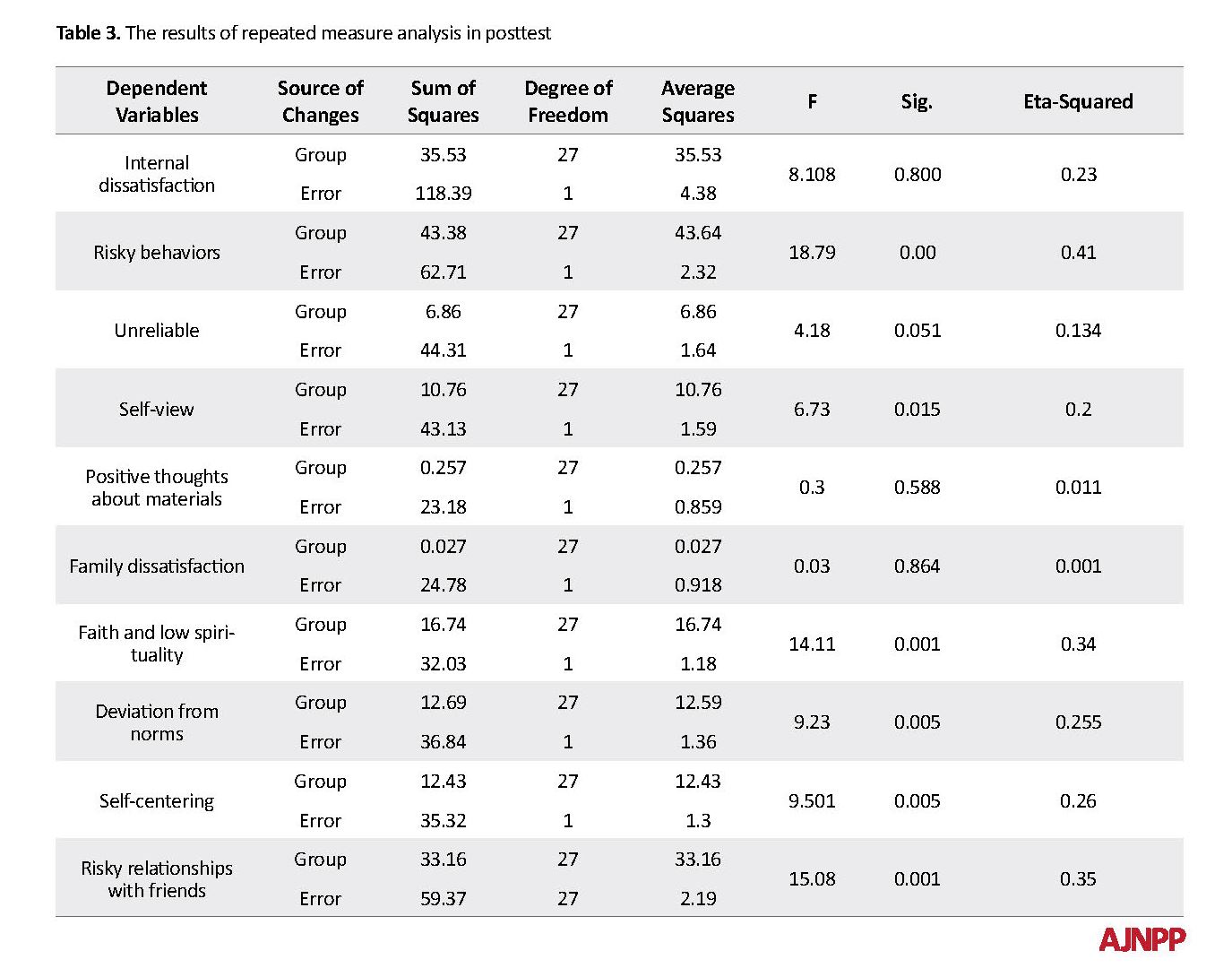
The Mean±SD of the students was 13.6±4.4 and 13.1±4.0 in the experimental group and the control group, respectively. According to the M box test, F equals 0.996 and the significance level of the test equals 48.33; so, the null hypothesis based on matrix homogeneity and variance of the covariance of DBT and control is confirmed (Table 2). The interactive effects (group and sub-scales of susceptible addiction pretest) in the posttest stage have higher levels than the 5% error (P>0.05); so, the assumption of homogeneity of regression slopes is also established. It is possible to use a repeated measure analysis (Table 3). Significant levels for Leven’s test in each subscale are more than 5% error; so, the assumption of homogeneity of error variances is acceptable for the control group and the experimental group.
After controlling the effect of the pretest, there was a significant difference between the experimental group and the control group. In other words, DBT therapeutic methods significantly affected the indicators of internal dissatisfaction, risk behaviors, self-view, deviation from the norms, self-centering, and relationships with friends in the posttest. Only 3 factors were unreliable; there was no significant difference between the positive thoughts and the family dissatisfaction. Insecurity, positive thoughts, and family dissatisfaction were not significant. Considering the Eta-squared, the most effective sub-scale was risk behaviors (0.49%) and the least effective sub-scale was self-view (0.2%).
4. Discussion
The result of this study is consistent with the study of Beckstead et al. [4]. According to the DBT approach, an individual with emotional problems cannot comprehend the totality of his or her emotions and experiences, is confused with them, and hardly can avoid them. In this study, with the training of decisiveness and conflict resolution in interpersonal skills, and in the model of stress tolerance, focusing on distress tolerance strategies, attention, and relaxation; in emotional regulation using the techniques of recognition and description of emotion, acceptance of traumatic experiences causing them to react and reducing their positive emotions; increasing adaptive behaviors and ability to perceive while reducing cognitive and maladaptive behaviors and ultimately reducing internal dissatisfaction, risky behaviors, self-view, deviance from norms, self-centered and risky relationships with friends.
4. Discussion
The result of this study is consistent with the study of Beckstead et al. [4]. According to the DBT approach, an individual with emotional problems cannot comprehend the totality of his or her emotions and experiences, is confused with them, and hardly can avoid them. In this study, with the training of decisiveness and conflict resolution in interpersonal skills, and in the model of stress tolerance, focusing on distress tolerance strategies, attention, and relaxation; in emotional regulation using the techniques of recognition and description of emotion, acceptance of traumatic experiences causing them to react and reducing their positive emotions; increasing adaptive behaviors and ability to perceive while reducing cognitive and maladaptive behaviors and ultimately reducing internal dissatisfaction, risky behaviors, self-view, deviance from norms, self-centered and risky relationships with friends.
Only 3 factors of unreliability, positive thoughts, and family dissatisfaction are not significant. Therefore, the use of the DBT technique leads to departing from emotions, understanding their totality, and mastering them. Also, DBT uses identifying techniques, the discovery of values, committed action, identifying superior power, and better communication with superior power, as advanced skills in tolerating distress help individuals to deal with a critical position more effectively [15].
Values, personal morality, human principles, and ideals are criteria or universal morals that can provide us with powerful ways to withstand stressful situations. Essential components in the life of individuals include family, romantic relationships, parenting, friendship, social life, citizenship, employment, education, leisure and entertainment, spirituality and religion, and self-care. We are endeavoring to work hard because of these values. Recognizing superior power and better communication with superior power lead to greater self-confidence and power. Believing in a superior power, in the way we are distressed by close people, or in unpredictable situations, such as the victim of crime, the accident, the death of loved ones, and infected with a deadly disease helps people to achieve a better life shortly. Changing positive attitudes, or stabilizing negative attitudes toward drugs, strengthening religious beliefs and religious values, teaching coping skills, informing students about drug complications and teaching life skills, enhancing self-esteem, self-confidence, self-control, daring, identity, and the emotional regulation of the adolescent are personal factors about drug use [16, 17].
The main focus of DBT is learning to reduce emotional responsiveness and emotional response [18]. All DBT skills target the emotional regulation, including observation, description, and automated and non-judgmental participation, and focus awareness on the present moment and effectiveness (rather than being correct) [18, 19]. The main emphasis of DBT is in the consciousness and subtlety of emotional suffering. As a natural progression to the skills of mindfulness, distress tolerance skills include the ability to experience and view emotions without trying to change or control emotional experiences, arousal, or distress. The principle of distress tolerance skills seeks to reduce the response of emotionally inappropriate behaviors (for example, impulsivity and secondary negative emotions) to emotional responses without changing their emotional responsiveness [20, 21]. While distress tolerance skills focus on tolerating exhilarating excitement, emotional regulation skills, on the other hand, reduce emotional disturbance by targeting the initial excitement in a non-judgmental environment and employing specific skills [22, 23]. Emotional adjustment skills emphasize the adjustment of intense excitement [24, 25].
This research was conducted in Tonekabon, where the generalization of the results to another society requires more extensive research. Some students did not cooperate inadvertently because of the lack of adequate time, the limitations of human behavior, and uncontrolled variables that were difficult to identify and control despite the author’s attempt. The limitations of the study include the lack of educational technology facilities at the school venue and the time limit for the implementation of the research. It is suggested that screening based on parents’ addiction scores should be conducted in kindergartens for detecting children at risk of the disease. Educational and interventional programs should be conducted continuously and in different stages based on the characteristics of each stage and about the students’ perceptual power. Interventional and educational programs for preventing addiction are family-centered and school-based and create a sense of belonging to people about family and school. It is recommended that the DBT method with other psychological therapies should be compared and studied in this statistical population. This approach should be considered on the subjects of older ages or people with other disorders and problems. Variables such as age, background, and evidence in the field of study should also be monitored to provide more accurate results. A similar study should be conducted at other primary levels so that it could be more confident about the results of the study. A similar study should be conducted at all levels among girls and boys.
5. Conclusion
DBT is effective in the components of addiction-prone male junior high school students.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages and signed the informed consent. They were also assured about the confidentiality of their information; moreover, they were allowed to leave the study whenever they wish and, if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization: Shekoufeh Rostami Nezhad; Methodology: Marzieh Arefi; Investigation: Shekoufeh Rostami Nezhad; Supervision: Ali Khademi, Writing-original draft: Shekoufeh Rostami Nezhad; Writing-review & editing, Funding acquisition, Resources: All author.
Conflict of interest
The authors declared no conflict of interest.
References
Ahovan M, Balali S, Shargh NA, Doostian Y. Efficacy of dialectical behavior therapy on clinical signs and emotion regulation in patients with obsessive-compulsive disorder. Mediterranean Journal of Social Sciences. 2016; 7(4):412-9. [DOI:10.5901/mjss.2016.v7n4p412]
Neacsiu AD, Eberle JW, Kramer R, Wiesmann T, Linehan MM. Dialectical behavior therapy skills for transdiagnostic emotion dysregulation: A pilot randomized controlled trial. Behaviour Research and Therapy. 2014; 59:40-51. [DOI:10.1016/j.brat.2014.05.005] [PMID]
Axelrod SR, Perepletchikova F, Holtzman K, Sinha R. Emotion regulation and substance use frequency in women with substance dependence and borderline personality disorder receiving dialectical behavior therapy. The American Journal of Drug and Alcohol Abuse. 2011; 37(1):37-42. [DOI:10.3109/00952990.2010.535582] [PMID] [PMCID]
Beckstead DJ, Lambert MJ, DuBose AP, Linehan M. Dialectical behavior therapy with American Indian/Alaska Native adolescents diagnosed with substance use disorders: Combining an evidence based treatment with cultural, traditional, and spiritual beliefs. Addictive behaviors. 2015; 51:84-7. [DOI:10.1016/j.addbeh.2015.07.018] [PMID]
Linehan MM, Korslund KE, Harned MS, Gallop RJ, Lungu A, Neacsiu AD, McDavid J, Comtois KA, Murray-Gregory AM. Dialectical behavior therapy for high suicide risk in individuals with borderline personality disorder: A randomized clinical trial and component analysis. JAMA Psychiatry. 2015; 72(5):475-82. [DOI:10.1001/jamapsychiatry.2014.3039] [PMID]
Courbasson C, Nishikawa Y, Dixon L. Outcome of dialectical behaviour therapy for concurrent eating and substance use disorders. Clinical Psychology & Psychotherapy. 2012; 19(5):434-49. [DOI:10.1002/cpp.748] [PMID]
Fleischhaker C, Böhme R, Sixt B, Brück C, Schneider C, Schulz E. Dialectical behavioral therapy for adolescents (DBT-A): A clinical trial for patients with suicidal and self-injurious behavior and borderline symptoms with a one-year follow-up. Child and Adolescent Psychiatry and Mental Health. 2011; 5(1):3. [DOI:10.1186/1753-2000-5-3] [PMID] [PMCID]
Gutteling BM, Montagne B, Nijs M, van den Bosch LW. Dialectical behavior therapy: Is outpatient group psychotherapy an effective alternative to individual psychotherapy? Preliminary conclusions. Comprehensive Psychiatry. 2012; 53(8):1161-8. [DOI:10.1016/j.comppsych.2012.03.017] [PMID]
McCay E, Carter C, Aiello A, Quesnel S, Langley J, Hwang S, et al. Dialectical behavior therapy as a catalyst for change in street-involved youth: A mixed methods study. Children and Youth Services Review. 2015; 58:187-99. [DOI:10.1016/j.childyouth.2015.09.021]
Anestis JC, Charles NE, Lee-Rowland LM, Barry CT, Gratz KL. Implementing dialectical behavior therapy skills training with at-risk male youth in a military-style residential program. Cognitive and Behavioral Practice. 2019; In Press. [DOI:10.1016/j.cbpra.2019.07.001]
Perepletchikova F, Axelrod SR, Kaufman J, Rounsaville BJ, Douglas‐Palumberi H, Miller AL. Adapting dialectical behaviour therapy for children: Towards a new research agenda for paediatric suicidal and non‐suicidal self‐injurious behaviours. Child and Adolescent Mental Health. 2011; 16(2):116-21. [DOI:10.1111/j.1475-3588.2010.00583.x] [PMID] [PMCID]
Rizvi SL, Steffel LM, Carson-Wong A. An overview of dialectical behavior therapy for professional psychologists. Professional Psychology: Research and Practice. 2013; 44(2):73. [DOI:10.1037/a0029808]
Wilks CR, Lungu A, Ang SY, Matsumiya B, Yin Q, Linehan MM. A randomized controlled trial of an Internet delivered dialectical behavior therapy skills training for suicidal and heavy episodic drinkers. Journal of Affective Disorders. 2018; 232:219-28. [DOI:10.1016/j.jad.2018.02.053] [PMID] [PMCID]
Shelton D, Kesten K, Zhang W, Trestman R. Impact of a dialectic behavior therapy-Corrections Modified (DBT‐CM) upon behaviorally challenged incarcerated male adolescents. Journal of Child and Adolescent Psychiatric Nursing. 2011; 24(2):105-13. [DOI:10.1111/j.1744-6171.2011.00275.x] [PMID] [PMCID]
Swales MA. Dialectical behaviour therapy: Description, research and future directions. International Journal of Behavioral Consultation and Therapy. 2009; 5(2):164-77. [DOI:10.1037/h0100878]
Felton JW, Shadur JM, Havewala M, Gonçalves S, Lejuez CW. Impulsivity moderates the relation between depressive symptoms and substance use across adolescence. Journal of Clinical Child & Adolescent Psychology. 2019; 15:1-13. [DOI:10.1080/15374416.2018.1537189] [PMID]
Martinez E, Tatum KL, Glass M, Bernath A, Ferris D, Reynolds P, et al. Correlates of smoking cessation self-efficacy in a community sample of smokers. Addictive Behaviors. 2010; 35(2):175-8. [DOI:10.1016/j.addbeh.2009.09.016] [PMID] [PMCID]
Koffarnus MN, Kaplan BA. Clinical models of decision making in addiction. Pharmacology Biochemistry and Behavior. 2018; 164:71-83. [DOI:10.1016/j.pbb.2017.08.010] [PMID] [PMCID]
Kim E, Yim HW, Jeong H, Jo SJ, Lee HK, Son HJ, et al. The association between aggression and risk of Internet gaming disorder in Korean adolescents: The mediation effect of father-adolescent communication style. Epidemiology and Health. 2018; 40:e2018039. [DOI:10.4178/epih.e2018039] [PMID] [PMCID]
Ougrin D, Zundel T, Kyriakopoulos M, Banarsee R, Stahl D, Taylor E. Adolescents with suicidal and nonsuicidal self-harm: Clinical characteristics and response to therapeutic assessment. Psychological Assessment. 2012; 24(1):11-20. https://psycnet.apa.org/doi/10.1037/a0025043 [DOI:10.1037/a0025043] [PMID]
Rizvi SL, Dimeff LA, Skutch J, Carroll D, Linehan MM. A pilot study of the DBT coach: An interactive mobile phone application for individuals with borderline personality disorder and substance use disorder. Behavior Therapy. 2011; 42(4):589-600. [DOI:10.1016/j.beth.2011.01.003] [PMID]
Olino TM, Benini L, Icenogle G, Wilson S, Klein DN, Seeley JR, et al. Is the assessment of personality comparable in persons who have and have not experienced depressive, anxiety, and substance use disorders? An examination of measurement invariance. Assessment. 2019; 26(1):45-55. [DOI:10.1177%2F1073191117725171] [PMID] [PMCID]
Dunne EM, Norris AL, Romer D, DiClemente RJ, Vanable PA, Valois RF, et al. Problem solving reduces sexual risk associated with sensation seeking, substance use, and depressive symptoms among African-American Adolescents. Journal of Child & Adolescent Substance Abuse. 2019; 28(2):113-8. [DOI:10.1080/1067828X.2019.1610679]
Hosier SG, Cox WM. Personality and motivational correlates of alcohol consumption and alcohol-related problems among excessive drinking university students. Addictive Behaviors. 2011; 36(1-2):87-94. [DOI:10.1016/j.addbeh.2010.08.029] [PMID]
Stotts AL, Northrup TF. The promise of third-wave behavioral therapies in the treatment of substance use disorders. Current Opinion in Psychology. 2015; 2:75-81. [DOI:10.1016/j.copsyc.2014.12.028] [PMID] [PMCID]
Values, personal morality, human principles, and ideals are criteria or universal morals that can provide us with powerful ways to withstand stressful situations. Essential components in the life of individuals include family, romantic relationships, parenting, friendship, social life, citizenship, employment, education, leisure and entertainment, spirituality and religion, and self-care. We are endeavoring to work hard because of these values. Recognizing superior power and better communication with superior power lead to greater self-confidence and power. Believing in a superior power, in the way we are distressed by close people, or in unpredictable situations, such as the victim of crime, the accident, the death of loved ones, and infected with a deadly disease helps people to achieve a better life shortly. Changing positive attitudes, or stabilizing negative attitudes toward drugs, strengthening religious beliefs and religious values, teaching coping skills, informing students about drug complications and teaching life skills, enhancing self-esteem, self-confidence, self-control, daring, identity, and the emotional regulation of the adolescent are personal factors about drug use [16, 17].
The main focus of DBT is learning to reduce emotional responsiveness and emotional response [18]. All DBT skills target the emotional regulation, including observation, description, and automated and non-judgmental participation, and focus awareness on the present moment and effectiveness (rather than being correct) [18, 19]. The main emphasis of DBT is in the consciousness and subtlety of emotional suffering. As a natural progression to the skills of mindfulness, distress tolerance skills include the ability to experience and view emotions without trying to change or control emotional experiences, arousal, or distress. The principle of distress tolerance skills seeks to reduce the response of emotionally inappropriate behaviors (for example, impulsivity and secondary negative emotions) to emotional responses without changing their emotional responsiveness [20, 21]. While distress tolerance skills focus on tolerating exhilarating excitement, emotional regulation skills, on the other hand, reduce emotional disturbance by targeting the initial excitement in a non-judgmental environment and employing specific skills [22, 23]. Emotional adjustment skills emphasize the adjustment of intense excitement [24, 25].
This research was conducted in Tonekabon, where the generalization of the results to another society requires more extensive research. Some students did not cooperate inadvertently because of the lack of adequate time, the limitations of human behavior, and uncontrolled variables that were difficult to identify and control despite the author’s attempt. The limitations of the study include the lack of educational technology facilities at the school venue and the time limit for the implementation of the research. It is suggested that screening based on parents’ addiction scores should be conducted in kindergartens for detecting children at risk of the disease. Educational and interventional programs should be conducted continuously and in different stages based on the characteristics of each stage and about the students’ perceptual power. Interventional and educational programs for preventing addiction are family-centered and school-based and create a sense of belonging to people about family and school. It is recommended that the DBT method with other psychological therapies should be compared and studied in this statistical population. This approach should be considered on the subjects of older ages or people with other disorders and problems. Variables such as age, background, and evidence in the field of study should also be monitored to provide more accurate results. A similar study should be conducted at other primary levels so that it could be more confident about the results of the study. A similar study should be conducted at all levels among girls and boys.
5. Conclusion
DBT is effective in the components of addiction-prone male junior high school students.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages and signed the informed consent. They were also assured about the confidentiality of their information; moreover, they were allowed to leave the study whenever they wish and, if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization: Shekoufeh Rostami Nezhad; Methodology: Marzieh Arefi; Investigation: Shekoufeh Rostami Nezhad; Supervision: Ali Khademi, Writing-original draft: Shekoufeh Rostami Nezhad; Writing-review & editing, Funding acquisition, Resources: All author.
Conflict of interest
The authors declared no conflict of interest.
References
Ahovan M, Balali S, Shargh NA, Doostian Y. Efficacy of dialectical behavior therapy on clinical signs and emotion regulation in patients with obsessive-compulsive disorder. Mediterranean Journal of Social Sciences. 2016; 7(4):412-9. [DOI:10.5901/mjss.2016.v7n4p412]
Neacsiu AD, Eberle JW, Kramer R, Wiesmann T, Linehan MM. Dialectical behavior therapy skills for transdiagnostic emotion dysregulation: A pilot randomized controlled trial. Behaviour Research and Therapy. 2014; 59:40-51. [DOI:10.1016/j.brat.2014.05.005] [PMID]
Axelrod SR, Perepletchikova F, Holtzman K, Sinha R. Emotion regulation and substance use frequency in women with substance dependence and borderline personality disorder receiving dialectical behavior therapy. The American Journal of Drug and Alcohol Abuse. 2011; 37(1):37-42. [DOI:10.3109/00952990.2010.535582] [PMID] [PMCID]
Beckstead DJ, Lambert MJ, DuBose AP, Linehan M. Dialectical behavior therapy with American Indian/Alaska Native adolescents diagnosed with substance use disorders: Combining an evidence based treatment with cultural, traditional, and spiritual beliefs. Addictive behaviors. 2015; 51:84-7. [DOI:10.1016/j.addbeh.2015.07.018] [PMID]
Linehan MM, Korslund KE, Harned MS, Gallop RJ, Lungu A, Neacsiu AD, McDavid J, Comtois KA, Murray-Gregory AM. Dialectical behavior therapy for high suicide risk in individuals with borderline personality disorder: A randomized clinical trial and component analysis. JAMA Psychiatry. 2015; 72(5):475-82. [DOI:10.1001/jamapsychiatry.2014.3039] [PMID]
Courbasson C, Nishikawa Y, Dixon L. Outcome of dialectical behaviour therapy for concurrent eating and substance use disorders. Clinical Psychology & Psychotherapy. 2012; 19(5):434-49. [DOI:10.1002/cpp.748] [PMID]
Fleischhaker C, Böhme R, Sixt B, Brück C, Schneider C, Schulz E. Dialectical behavioral therapy for adolescents (DBT-A): A clinical trial for patients with suicidal and self-injurious behavior and borderline symptoms with a one-year follow-up. Child and Adolescent Psychiatry and Mental Health. 2011; 5(1):3. [DOI:10.1186/1753-2000-5-3] [PMID] [PMCID]
Gutteling BM, Montagne B, Nijs M, van den Bosch LW. Dialectical behavior therapy: Is outpatient group psychotherapy an effective alternative to individual psychotherapy? Preliminary conclusions. Comprehensive Psychiatry. 2012; 53(8):1161-8. [DOI:10.1016/j.comppsych.2012.03.017] [PMID]
McCay E, Carter C, Aiello A, Quesnel S, Langley J, Hwang S, et al. Dialectical behavior therapy as a catalyst for change in street-involved youth: A mixed methods study. Children and Youth Services Review. 2015; 58:187-99. [DOI:10.1016/j.childyouth.2015.09.021]
Anestis JC, Charles NE, Lee-Rowland LM, Barry CT, Gratz KL. Implementing dialectical behavior therapy skills training with at-risk male youth in a military-style residential program. Cognitive and Behavioral Practice. 2019; In Press. [DOI:10.1016/j.cbpra.2019.07.001]
Perepletchikova F, Axelrod SR, Kaufman J, Rounsaville BJ, Douglas‐Palumberi H, Miller AL. Adapting dialectical behaviour therapy for children: Towards a new research agenda for paediatric suicidal and non‐suicidal self‐injurious behaviours. Child and Adolescent Mental Health. 2011; 16(2):116-21. [DOI:10.1111/j.1475-3588.2010.00583.x] [PMID] [PMCID]
Rizvi SL, Steffel LM, Carson-Wong A. An overview of dialectical behavior therapy for professional psychologists. Professional Psychology: Research and Practice. 2013; 44(2):73. [DOI:10.1037/a0029808]
Wilks CR, Lungu A, Ang SY, Matsumiya B, Yin Q, Linehan MM. A randomized controlled trial of an Internet delivered dialectical behavior therapy skills training for suicidal and heavy episodic drinkers. Journal of Affective Disorders. 2018; 232:219-28. [DOI:10.1016/j.jad.2018.02.053] [PMID] [PMCID]
Shelton D, Kesten K, Zhang W, Trestman R. Impact of a dialectic behavior therapy-Corrections Modified (DBT‐CM) upon behaviorally challenged incarcerated male adolescents. Journal of Child and Adolescent Psychiatric Nursing. 2011; 24(2):105-13. [DOI:10.1111/j.1744-6171.2011.00275.x] [PMID] [PMCID]
Swales MA. Dialectical behaviour therapy: Description, research and future directions. International Journal of Behavioral Consultation and Therapy. 2009; 5(2):164-77. [DOI:10.1037/h0100878]
Felton JW, Shadur JM, Havewala M, Gonçalves S, Lejuez CW. Impulsivity moderates the relation between depressive symptoms and substance use across adolescence. Journal of Clinical Child & Adolescent Psychology. 2019; 15:1-13. [DOI:10.1080/15374416.2018.1537189] [PMID]
Martinez E, Tatum KL, Glass M, Bernath A, Ferris D, Reynolds P, et al. Correlates of smoking cessation self-efficacy in a community sample of smokers. Addictive Behaviors. 2010; 35(2):175-8. [DOI:10.1016/j.addbeh.2009.09.016] [PMID] [PMCID]
Koffarnus MN, Kaplan BA. Clinical models of decision making in addiction. Pharmacology Biochemistry and Behavior. 2018; 164:71-83. [DOI:10.1016/j.pbb.2017.08.010] [PMID] [PMCID]
Kim E, Yim HW, Jeong H, Jo SJ, Lee HK, Son HJ, et al. The association between aggression and risk of Internet gaming disorder in Korean adolescents: The mediation effect of father-adolescent communication style. Epidemiology and Health. 2018; 40:e2018039. [DOI:10.4178/epih.e2018039] [PMID] [PMCID]
Ougrin D, Zundel T, Kyriakopoulos M, Banarsee R, Stahl D, Taylor E. Adolescents with suicidal and nonsuicidal self-harm: Clinical characteristics and response to therapeutic assessment. Psychological Assessment. 2012; 24(1):11-20. https://psycnet.apa.org/doi/10.1037/a0025043 [DOI:10.1037/a0025043] [PMID]
Rizvi SL, Dimeff LA, Skutch J, Carroll D, Linehan MM. A pilot study of the DBT coach: An interactive mobile phone application for individuals with borderline personality disorder and substance use disorder. Behavior Therapy. 2011; 42(4):589-600. [DOI:10.1016/j.beth.2011.01.003] [PMID]
Olino TM, Benini L, Icenogle G, Wilson S, Klein DN, Seeley JR, et al. Is the assessment of personality comparable in persons who have and have not experienced depressive, anxiety, and substance use disorders? An examination of measurement invariance. Assessment. 2019; 26(1):45-55. [DOI:10.1177%2F1073191117725171] [PMID] [PMCID]
Dunne EM, Norris AL, Romer D, DiClemente RJ, Vanable PA, Valois RF, et al. Problem solving reduces sexual risk associated with sensation seeking, substance use, and depressive symptoms among African-American Adolescents. Journal of Child & Adolescent Substance Abuse. 2019; 28(2):113-8. [DOI:10.1080/1067828X.2019.1610679]
Hosier SG, Cox WM. Personality and motivational correlates of alcohol consumption and alcohol-related problems among excessive drinking university students. Addictive Behaviors. 2011; 36(1-2):87-94. [DOI:10.1016/j.addbeh.2010.08.029] [PMID]
Stotts AL, Northrup TF. The promise of third-wave behavioral therapies in the treatment of substance use disorders. Current Opinion in Psychology. 2015; 2:75-81. [DOI:10.1016/j.copsyc.2014.12.028] [PMID] [PMCID]
Article Type: Research Article |
Subject:
Substance abuse, dependence, addiction
Received: 2018/07/15 | Accepted: 2018/11/1 | Published: 2019/02/1
Received: 2018/07/15 | Accepted: 2018/11/1 | Published: 2019/02/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Hamadan University of Medical Sciences.
Published by UMSHA Press
Journal Tel: +989025126654
Publisher Tel: +985138419434
Website: http://ajnpp.umsha.ac.ir
Email: avicennajnpp[at]gmail.com
