

Volume 7, Issue 1 (February 2020)
Avicenna J Neuro Psycho Physiology 2020, 7(1): 29-36 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ismaeilzadeh N, Akbari B. Effectiveness of Mindfulness-Based Cognitive Therapy in Sexual Self-Efficacy and Marital Satisfaction among Couples with Marital Conflicts. Avicenna J Neuro Psycho Physiology 2020; 7 (1) :29-36
URL: http://ajnpp.umsha.ac.ir/article-1-308-en.html
URL: http://ajnpp.umsha.ac.ir/article-1-308-en.html



1- PhD Student, General Psychology, Department of Psychology, Rasht Branch, Islamic Azad University, Rasht, Iran
2- Associate Professor, Department of Psychology, Rasht Branch, Islamic Azad University, Rasht, Iran , akbari@iaurasht.ac.ir
2- Associate Professor, Department of Psychology, Rasht Branch, Islamic Azad University, Rasht, Iran , akbari@iaurasht.ac.ir
Full-Text [PDF 1771 kb]
(994 Downloads)
| Abstract (HTML) (1975 Views)
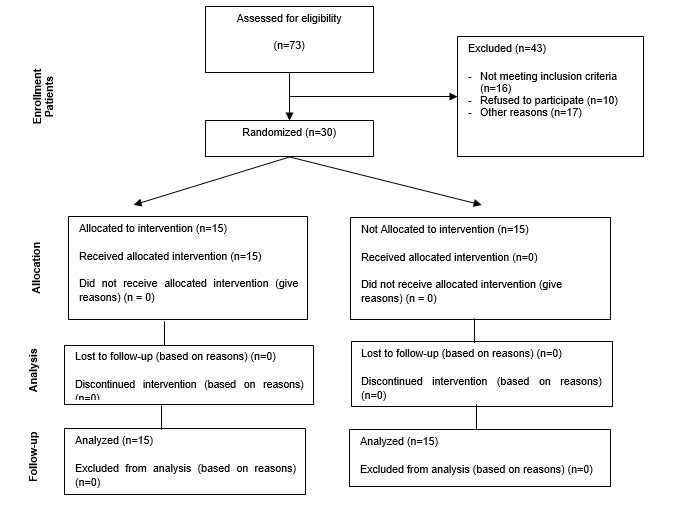
Table 2. Descriptive results of sexual self-efficacy scale in intervention and control groups
Table 3. Multivariate analysis of variance of dependent variables in control and intervention groups
Table 4. Results of multivariate analysis of covariance regarding impact of mindfulness-based cognitive therapy on marital satisfaction
Full-Text: (1455 Views)
Background
A satisfying sexual relationship is a part of the intimate relationship of couples and strong correlate of marital satisfaction [1]. Sexual satisfaction, as one of the elements of marital satisfaction, is an important index for a successful marriage and survival and health of the family [2]. It defines a couple’s satisfaction with their sexual relationship and their ability to enjoy themselves and each other [3, 4]. This issue is not only associated with physical pleasure but also includes all of the emotions regarding positive and negative sexual relationships [5, 6]. Sexual dissatisfaction has been proposed to be associated with triggering many psychosomatic symptoms, including migraine headaches, symptoms of premenstrual syndrome, chronic arthritis, and complex marital problems, in couples’ relationships [7, 8].
Marital conflict is a type of lack of ongoing meaningful agreement between the spouses. Meaningfulness refers to the effect of this problem on the performance of spouses, and consistency denotes the differences not disappearing with the lapse of time [3]. The fact is that the occurrence of marital conflicts is an inevitable phenomenon in any normal life, and couples need to learn to resolve their marital conflicts to have a happy life [4].
The results of previous studies showed that couples who manage their marital conflicts using positive methods and less negative interactions create an atmosphere in which they have a higher chance of self-disclosure and agreement concerning family problems [5]. According to the evidence, it was indicated that couples with poor sexual performance and self-efficacy [6] have a lower level of marital satisfaction [7], suffer from early maladaptive schemas [8], and report higher levels of marital conflicts threatening the health of marital life and in acute cases leading to divorce [9].
It seems that many Iranian couples are suffering from sexual dissatisfaction; however, shame, embarrassment, or distress might prohibit them from discussing their concerns with either a psychologist or physician [9]. Learning the necessary skills for having a satisfactory sexual relationship could be achieved by the provision of appropriate education for couples. In addition, counseling programs provided by well-educated health professionals might increase couples’ sexual satisfaction [10].
By providing counseling, education, and necessary information about the physiology of an individual’s sexual response, the associated problems would gradually be resolved, and the couples would be able to effectively and successfully encounter their sexual problems [11]. Therefore, it is important to evaluate the condition of sexual relationships which has an important role in creating a pleasant marital life [12]. To date, various methods, including interactive behavior analysis, interventions based on the cognitive-behavioral theory of choice, solution-oriented counseling, emotion-focused treatment, and mindfulness-based cognitive therapy, have been used for increasing the sexual satisfaction of couples [13].
One of the treatment methods is mindfulness-based cognitive therapy as one of the most modern developments in cognitive therapies. In this regard, using new family therapy techniques, such as mindfulness-based cognitive therapy, has a significant role in the reduction of marital conflicts. Mindfulness techniques employing mindfulness-based exercises, encouraging attention, and promoting nonjudgmental observations and acceptance of physical feelings, perceptions, cognitions, and emotions lead to a reduction of marital conflicts resulting from inappropriate sexual performance, maladaptive schemas, and marital satisfaction [14].
By the application of the mindfulness-based training technique, couples will learn to consider the above-mentioned cases with interest and curiosity, accept them as they are, and eventually understand that although marital problems may happen, there are also new ways to deal with these issues. The core of this method is mindfulness, and as a result it is expected that those in the intervention group will be able to enhance their marital satisfaction, reduce early maladaptive schemes, and increase their sexual self-efficacy by learning new ideas and replacing these ideas with behavioral modification skills as well as acceptance of others.
Regarding cultural issues related to sexual matters in Iran, such as the lack of sufficient information in this regard and existence of inappropriate beliefs and attitudes towards this issue, the debate on women’s sexual activity is considered a cultural taboo. This issue among the families, especially the newly married couples, has resulted in the destruction of many families [15, 16]. In this
regard, the researchers are investigating whether mindfulness-based cognitive therapy is effective in other countries, such as Iran.
Objectives
This study aimed to evaluate the effectiveness of mindfulness-based cognitive therapy on sexual self-efficacy and marital satisfaction in couples with marital conflicts.
Materials and Methods
This quasi-experimental study was carried on two intervention and control groups with a pretest/posttest design and follow-up. The study population consisted of 30 women referring to Bahar, Negah No, Pasargad, and Ehya counseling centers in district 1 of Tehran, Iran, during 3-6 months in 2018 through simple random sampling. The participants were randomly divided into two groups, each with 15 members. The control and intervention groups were also matched and controlled regarding age (range: 25-35 years), educational level (all with university degrees), and duration of the marriage.
After assigning the subjects to the intervention and control groups, the questionnaires of sexual self-efficacy, marital satisfaction, and marital conflicts were distributed between the two groups before and after the training period of mindfulness-based cognitive therapy, and the obtained scores were evaluated. It should be noted that the follow-up phase was conducted after 3 months. The inclusion criteria were the age range of 25-35 years, university degree, and marriage duration of 3-10 years. The exclusion criteria were the age of under 25 and over 35 years, no academic degree, and marriage duration of under 3 years and over 10 years.
The ethical considerations were considered, including the participants’ freedom to cooperate or withdraw the survey at any time. The researcher explained scientific reasoning for the study subjects. They were ensured that any information given during the interview would be confidential. It was essential to establish that their intellectual property would be preserved when the results of the study were published. The participants attended the experiment entirely without paying any costs. After the end of the study, the treatment was performed on the control group. Mindfulness-based cognitive therapy training was conducted within eight 60-minute sessions focusing on the topics shown in Table 1.
Marital conflict is a type of lack of ongoing meaningful agreement between the spouses. Meaningfulness refers to the effect of this problem on the performance of spouses, and consistency denotes the differences not disappearing with the lapse of time [3]. The fact is that the occurrence of marital conflicts is an inevitable phenomenon in any normal life, and couples need to learn to resolve their marital conflicts to have a happy life [4].
The results of previous studies showed that couples who manage their marital conflicts using positive methods and less negative interactions create an atmosphere in which they have a higher chance of self-disclosure and agreement concerning family problems [5]. According to the evidence, it was indicated that couples with poor sexual performance and self-efficacy [6] have a lower level of marital satisfaction [7], suffer from early maladaptive schemas [8], and report higher levels of marital conflicts threatening the health of marital life and in acute cases leading to divorce [9].
It seems that many Iranian couples are suffering from sexual dissatisfaction; however, shame, embarrassment, or distress might prohibit them from discussing their concerns with either a psychologist or physician [9]. Learning the necessary skills for having a satisfactory sexual relationship could be achieved by the provision of appropriate education for couples. In addition, counseling programs provided by well-educated health professionals might increase couples’ sexual satisfaction [10].
By providing counseling, education, and necessary information about the physiology of an individual’s sexual response, the associated problems would gradually be resolved, and the couples would be able to effectively and successfully encounter their sexual problems [11]. Therefore, it is important to evaluate the condition of sexual relationships which has an important role in creating a pleasant marital life [12]. To date, various methods, including interactive behavior analysis, interventions based on the cognitive-behavioral theory of choice, solution-oriented counseling, emotion-focused treatment, and mindfulness-based cognitive therapy, have been used for increasing the sexual satisfaction of couples [13].
One of the treatment methods is mindfulness-based cognitive therapy as one of the most modern developments in cognitive therapies. In this regard, using new family therapy techniques, such as mindfulness-based cognitive therapy, has a significant role in the reduction of marital conflicts. Mindfulness techniques employing mindfulness-based exercises, encouraging attention, and promoting nonjudgmental observations and acceptance of physical feelings, perceptions, cognitions, and emotions lead to a reduction of marital conflicts resulting from inappropriate sexual performance, maladaptive schemas, and marital satisfaction [14].
By the application of the mindfulness-based training technique, couples will learn to consider the above-mentioned cases with interest and curiosity, accept them as they are, and eventually understand that although marital problems may happen, there are also new ways to deal with these issues. The core of this method is mindfulness, and as a result it is expected that those in the intervention group will be able to enhance their marital satisfaction, reduce early maladaptive schemes, and increase their sexual self-efficacy by learning new ideas and replacing these ideas with behavioral modification skills as well as acceptance of others.
Regarding cultural issues related to sexual matters in Iran, such as the lack of sufficient information in this regard and existence of inappropriate beliefs and attitudes towards this issue, the debate on women’s sexual activity is considered a cultural taboo. This issue among the families, especially the newly married couples, has resulted in the destruction of many families [15, 16]. In this
regard, the researchers are investigating whether mindfulness-based cognitive therapy is effective in other countries, such as Iran.
Objectives
This study aimed to evaluate the effectiveness of mindfulness-based cognitive therapy on sexual self-efficacy and marital satisfaction in couples with marital conflicts.
Materials and Methods
This quasi-experimental study was carried on two intervention and control groups with a pretest/posttest design and follow-up. The study population consisted of 30 women referring to Bahar, Negah No, Pasargad, and Ehya counseling centers in district 1 of Tehran, Iran, during 3-6 months in 2018 through simple random sampling. The participants were randomly divided into two groups, each with 15 members. The control and intervention groups were also matched and controlled regarding age (range: 25-35 years), educational level (all with university degrees), and duration of the marriage.
After assigning the subjects to the intervention and control groups, the questionnaires of sexual self-efficacy, marital satisfaction, and marital conflicts were distributed between the two groups before and after the training period of mindfulness-based cognitive therapy, and the obtained scores were evaluated. It should be noted that the follow-up phase was conducted after 3 months. The inclusion criteria were the age range of 25-35 years, university degree, and marriage duration of 3-10 years. The exclusion criteria were the age of under 25 and over 35 years, no academic degree, and marriage duration of under 3 years and over 10 years.
The ethical considerations were considered, including the participants’ freedom to cooperate or withdraw the survey at any time. The researcher explained scientific reasoning for the study subjects. They were ensured that any information given during the interview would be confidential. It was essential to establish that their intellectual property would be preserved when the results of the study were published. The participants attended the experiment entirely without paying any costs. After the end of the study, the treatment was performed on the control group. Mindfulness-based cognitive therapy training was conducted within eight 60-minute sessions focusing on the topics shown in Table 1.
Table 1. Content of mindfulness-based cognitive therapy sessions
| Session | Content |
| First | Body-checking exercises, mindfulness exercises, and 3-minute breathing exercises, all of which are examples of formal mindfulness exercises. The group was asked to choose an activity from daily activities and pay close attention to their own moment-to-moment sensory experiences during the week. During every single session, everyone was allowed to discuss and review these experiences. In practicing bodily senses, group members learned that a conscious focus on different parts of the body, while seemed to be simple and easy, gave them the ability to have control over the process of mental activity. Therefore, in body control exercise, the ability to focus on body parts and various ways of attention were expanded. By focusing on each part of the body, the members of the group were asked to imagine how the movement of air was during inhaling and exhaling, guiding the wind through the various parts, and controlling them in this way to help learn how to use the air as a tool to direct their attention. |
| Second | The members of the group were asked to record their daily experiences regarding desirable or pleasant events using a timetable. They should pay attention to what happened when an event occurred (i.e., what bodily feelings did they experience? what thoughts and mentalities did emerge? what emotional or feeling states did happen? Then, while recording an event, the members of the group were asked to write down their thoughts at that moment. The researchers received help from paying attention to their respiratory emotions, and as a result they used it to establish the mind in the present moment. This process of focusing on the particular details and dimensions of the experience helped to separate the participants from deep mental activities. |
| Third | During the third week, the members of the group were asked to do the same affairs, this time about unpleasant events. In this session, they recorded, analyzed, and reviewed experiences resulting from natural phenomena, such as staying behind traffic lights, cleaning the floor, or contacting customer service. During the meditation sessions, the skills of focus and attention were nurtured. Group members learned how to focus their thoughts. Fostering the ability to establish the mind paves the way to generate conscious and mindful awareness and provides a broader range of our experiences. |
| Fourth | The primary purpose of this recording exercise was to facilitate the understanding and perception of emotions, which is a combination of the consequences resulting from a situation plus an interpretation. The members of the group were invited to be in a relaxed state, close their eyes, and imagine themselves in an unpleasant situation. While imagining this picture, various responses of group members to the case indicate that our ultimate sense of a situation will be relatively directly determined by what we think. |
| Fifth | By merely adjusting their emotions, group members broke the chain of habitual reactions that were familiar to everyone, including unpleasant experiences, disgust, muscle contraction, and emotional stress resulting from events as well as negative thoughts rotation. The key to this debate is to move toward positive thinking and friendship with the events that occur at any given moment. They were asked to remember the unpleasant experience that still haunts them during the meditation session and experience these thoughts with their physical sensations. This process is a part of an overall movement to reinforce relationships and embrace the aspects of experiences that are marginalized and exert an influence upon individuals. It is not an effort to change the problems, but the desire and determination to maintain the reality as it is. Group members will also find out how often problems arise in mind and can be modified by changing their feelings about these issues and turning them into positive effects. This session will emphasize the need for feeling and experiencing things as they are, without judgment. |
| Sixth | The purpose of this session is to understand that not only what individuals think has an impact on their emotions but also emotions have an effect on thoughts. They learned that mindfulness skills provide an opportunity to break the chain of reactive responses by paying attention and focusing on the topics as well as developing the group members’ viewpoints. Giving information and reminding that the interpretations are influenced by various factors, such as past experiences or mental states, help individuals to be more careful when interpreting events. It can be assumed that interpretations are not necessarily representations of reality. Mindfulness can offer new ways to stay in the present, such as using sensory experiences, conscious breathing, and sitting meditation, which are performed by the group members at this session. |
| Seventh | Thoughts are not facts. The subjects that individuals think about are only thoughts, and people can choose not to act based on them or deal with them and consider them subjective altogether. In this session, the ways to get out of the negative mood and thoughts were taught to the members of the group, and they can use them as lenses and examine and observe their experiences more closely. This process of recognizing the existing patterns of thought can help ruminate by sitting meditation and seek other solutions. However, by reaching a broader perspective on the thinking process, individuals will be able to cognitively work on them with an attitude of inquiry. |
| Eighth | The group members learn that the process of focusing and paying attention to experiences is nothing but accurately paying attention to consistency in feeling, experiencing, and observing these experiences. All that is performed during mindfulness exercises is to understand the concept of avoiding constant repetitions and habitual behaviors. The first thing to be considered in performing these exercises is that individuals should set a specific goal and be oriented toward experiences. The purpose is to create awareness and mindfulness regarding the present reality and its resultant expertise and develop the desire and determination to maintain truth the way it is. Through employing this particular way of describing and recounting direct experiences, the members of the group learn that they should abandon their futile thinking about their experiences. Mindfulness guides individuals to purposeful and motivated attention to achieve the desired results. |
Sexual self-efficacy scale
The sexual self-efficacy questionnaire was developed by Vaziri and Lotfi Kashani based on Schwartzer’s general self-efficacy questionnaire. The questionnaire consisted of 10 items scored based on a four-choice continuum within the range of 0 (i.e., totally incorrect) to 3 (i.e., completely correct). In the preliminary research, the reliability of the sexual self-efficacy questionnaire using Cronbach’s alpha coefficient was reported as 0.86 [17]. The validity and reliability of the Iranian version of the sexual self-efficacy questionnaire were 0.77 and 0.81, respectively [17].
Marital satisfaction scale
Marital satisfaction questionnaire developed by Enrich et al. is used to measure the dimensions of marital satisfaction. The questionnaire consists of four scales, including ideal distortions, marital satisfaction, communication, and conflict resolution [18]. This questionnaire is rated on a 5-point Likert scale within the score range of 1-5 (i.e., strongly disagree to strongly agree). This scale measures a couple’s tendency to respond to the items based
on socially acceptable behaviors. A low score represents an unrealistic attitude toward marriage.
This scale measures the satisfaction and conformity of individuals with 10 aspects of the marital relationship, including personality issues, marital relationships, conflict resolution, financial management, leisure activities, sexual relations, marriage and children, relatives and friends, equality-seeking roles, and religious orientation. A high score indicates high marital satisfaction. The validity and reliability of this research instrument were investigated in a study carried out by Farnam et al. [19] for dimensions of marital satisfaction, communication, conflict resolution, idealistic distortion, and total marital satisfaction with the reported scores of 0.86, 0.90, 0.84, 0.83, and 0.95, respectively.
Marital conflicts questionnaire
This questionnaire is an instrument involving 42 5-choice items, with a Cronbach’s alpha coefficient of 0.53 calculated by Sanai and Barati. This questionnaire measures seven dimensions of marital conflicts, including the reduction of cooperation, sexual relationship, increase of emotional reactions, increase in child support, increase of personal relationships with relatives, decrease in family relationships with friends, and separation of financial affairs from each other. Answering the questions was based on the Likert scale, including never [1], rarely, sometimes, often, and always [5]. In this questionnaire, a higher score represents more conflicts. The reliability coefficients of the total score of the questionnaire calculated by Askari et al. [20] using Cronbach’s alpha and retest method were 0.52 and 0.92, respectively.
The SPSS software (version 20) and descriptive statistical methods, including the calculation of frequency, percentage, mean, and standard deviation, were used to analyze the data of the study. The collected data were analyzed by repeated measurement analysis and analysis of covariance (ANCOVA) in SPSS software (version 22).
The sexual self-efficacy questionnaire was developed by Vaziri and Lotfi Kashani based on Schwartzer’s general self-efficacy questionnaire. The questionnaire consisted of 10 items scored based on a four-choice continuum within the range of 0 (i.e., totally incorrect) to 3 (i.e., completely correct). In the preliminary research, the reliability of the sexual self-efficacy questionnaire using Cronbach’s alpha coefficient was reported as 0.86 [17]. The validity and reliability of the Iranian version of the sexual self-efficacy questionnaire were 0.77 and 0.81, respectively [17].
Marital satisfaction scale
Marital satisfaction questionnaire developed by Enrich et al. is used to measure the dimensions of marital satisfaction. The questionnaire consists of four scales, including ideal distortions, marital satisfaction, communication, and conflict resolution [18]. This questionnaire is rated on a 5-point Likert scale within the score range of 1-5 (i.e., strongly disagree to strongly agree). This scale measures a couple’s tendency to respond to the items based
on socially acceptable behaviors. A low score represents an unrealistic attitude toward marriage.
This scale measures the satisfaction and conformity of individuals with 10 aspects of the marital relationship, including personality issues, marital relationships, conflict resolution, financial management, leisure activities, sexual relations, marriage and children, relatives and friends, equality-seeking roles, and religious orientation. A high score indicates high marital satisfaction. The validity and reliability of this research instrument were investigated in a study carried out by Farnam et al. [19] for dimensions of marital satisfaction, communication, conflict resolution, idealistic distortion, and total marital satisfaction with the reported scores of 0.86, 0.90, 0.84, 0.83, and 0.95, respectively.
Marital conflicts questionnaire
This questionnaire is an instrument involving 42 5-choice items, with a Cronbach’s alpha coefficient of 0.53 calculated by Sanai and Barati. This questionnaire measures seven dimensions of marital conflicts, including the reduction of cooperation, sexual relationship, increase of emotional reactions, increase in child support, increase of personal relationships with relatives, decrease in family relationships with friends, and separation of financial affairs from each other. Answering the questions was based on the Likert scale, including never [1], rarely, sometimes, often, and always [5]. In this questionnaire, a higher score represents more conflicts. The reliability coefficients of the total score of the questionnaire calculated by Askari et al. [20] using Cronbach’s alpha and retest method were 0.52 and 0.92, respectively.
The SPSS software (version 20) and descriptive statistical methods, including the calculation of frequency, percentage, mean, and standard deviation, were used to analyze the data of the study. The collected data were analyzed by repeated measurement analysis and analysis of covariance (ANCOVA) in SPSS software (version 22).
Figure 1. CONSORT checklist diagram
Results
The subjects in this study were 30 women with the mean age values of 32.22±7.19 and 31.11±6.55 years for the intervention and control groups, respectively, indicating the homogeneity of the two groups in terms of age.
The results of the Shapiro-Wilk test showed that the data had a normal distribution, and parametric tests can be used. The results of Levene’s variance homogeneity test indicated that the assumption of homogeneity of the data was accepted (P>0.05). The results of repeated measure analysis of variance (ANOVA) demonstrated that intergroup differences regarding sexual self-efficacy and marital satisfaction had a significant effect on treatment duration (P>0.003).
According to the results of Table 3, the multivariate analysis of the differences between the control and intervention groups regarding the subscales of sexual self-efficacy and marital satisfaction was significant (Wilks’ Lambda: 0.459; P<0.002).
Table 4 shows the results of the multivariate ANCOVA after removing the pretest effect. The obtained findings revealed that mindfulness-based cognitive therapy had an effect on marital satisfaction (test coefficient [1, 24]: 5.10; P=0.033). Considering the amount of the mediating variable (i.e., mindfulness-based cognitive therapy) effect, it can be said that (eta coefficient: 0.175) mindfulness-based cognitive therapy training was effective in the promotion of marital satisfaction in the intervention group.
In the next dimension, after removing the effect of the pretest, mindfulness-based cognitive therapy had a significant impact on communication (test coefficient [1, 24]: 4.82; P=0.038). With regard to the amount of the mediating variable (i.e., mindfulness-based cognitive therapy) effect, it can be said that (eta coefficient: 0.167) mindfulness-based cognitive therapy training was effective in the enhancement of communication in the intervention group.
The subjects in this study were 30 women with the mean age values of 32.22±7.19 and 31.11±6.55 years for the intervention and control groups, respectively, indicating the homogeneity of the two groups in terms of age.
The results of the Shapiro-Wilk test showed that the data had a normal distribution, and parametric tests can be used. The results of Levene’s variance homogeneity test indicated that the assumption of homogeneity of the data was accepted (P>0.05). The results of repeated measure analysis of variance (ANOVA) demonstrated that intergroup differences regarding sexual self-efficacy and marital satisfaction had a significant effect on treatment duration (P>0.003).
According to the results of Table 3, the multivariate analysis of the differences between the control and intervention groups regarding the subscales of sexual self-efficacy and marital satisfaction was significant (Wilks’ Lambda: 0.459; P<0.002).
Table 4 shows the results of the multivariate ANCOVA after removing the pretest effect. The obtained findings revealed that mindfulness-based cognitive therapy had an effect on marital satisfaction (test coefficient [1, 24]: 5.10; P=0.033). Considering the amount of the mediating variable (i.e., mindfulness-based cognitive therapy) effect, it can be said that (eta coefficient: 0.175) mindfulness-based cognitive therapy training was effective in the promotion of marital satisfaction in the intervention group.
In the next dimension, after removing the effect of the pretest, mindfulness-based cognitive therapy had a significant impact on communication (test coefficient [1, 24]: 4.82; P=0.038). With regard to the amount of the mediating variable (i.e., mindfulness-based cognitive therapy) effect, it can be said that (eta coefficient: 0.167) mindfulness-based cognitive therapy training was effective in the enhancement of communication in the intervention group.
Table 2. Descriptive results of sexual self-efficacy scale in intervention and control groups
| Scale | Group | Control | Intervention (Mindfulness-based cognitive therapy) |
||
| Mean | Standard deviation | Mean | Standard deviation | ||
| Marital satisfaction | Pretest | 19.47 | 4.03 | 19.27 | 3.84 |
| Posttest | 23.20 | 3.43 | 26.60 | 3.60 | |
| Follow-up | 20.47 | 3.18 | 24.73 | 3.83 | |
| Communication | Pretest | 22.27 | 4.03 | 25.53 | 5.34 |
| Posttest | 23.83 | 4.27 | 29.60 | 4.45 | |
| Follow-up | 22.13 | 3.48 | 28.67 | 4.50 | |
| Conflict resolution | Pretest | 22.67 | 3.94 | 26.67 | 3.29 |
| Posttest | 24.67 | 3.72 | 29.27 | 4.27 | |
| Follow-up | 24.00 | 3.64 | 28.07 | 4.35 | |
| Idealistic distortion | Pretest | 8.27 | 2.60 | 9.00 | 1.89 |
| Posttest | 9.27 | 2.02 | 10.27 | 1.87 | |
| Follow-up | 7.60 | 1.96 | 9.67 | 1.99 | |
| Sexual self-efficacy | Pretest | 10.73 | 2.71 | 11.00 | 2.39 |
| Posttest | 10.87 | 3.02 | 14.13 | 2.72 | |
| Follow-up | 10.20 | 1.74 | 13.80 | 2.51 | |
Table 3. Multivariate analysis of variance of dependent variables in control and intervention groups
| Value | F | df | df Error | Sig. | |
| Pillai’s Trace | 0.541 | 6.176 | 5.00 | 20.00 | 0.002 |
| Wilks’ Lambda | 0.459 | 6.176 | 5.000 | 20.00 | 0.002 |
| Hotelling’s Trace | 1.176 | 6.176 | 5.000 | 20.00 | 0.002 |
| Roy’s Largest Root | 1.176 | 6.176 | 5.000 | 20.00 | 0.002 |
Table 4. Results of multivariate analysis of covariance regarding impact of mindfulness-based cognitive therapy on marital satisfaction
| Variable | SS | df | MS | F | P | Eta | |
| Group | Marital satisfaction | 38.778 | 1 | 38.778 | 5.096 | 0.033 | 0.175 |
| Communication | 31.288 | 1 | 31.288 | 4.825 | 0.038 | 0.167 | |
| Conflict resolution | 79.333 | 1 | 79.333 | 5.687 | 0.025 | 0.192 | |
| Idealistic resolution | 0.075 | 1 | 0.075 | 0.030 | 0.864 | 0.001 | |
| Sexual self-efficacy | 42.022 | 25 | 21.011 | 5.601 | 0.006 | 0.167 | |
| Error | Marital satisfaction | 182.627 | 25 | 7.609 | |||
| Communication | 155.617 | 25 | 6.484 | ||||
| Conflict resolution | 334.789 | 25 | 13.950 | ||||
| Idealistic resolution | 60.751 | 25 | 2.531 | ||||
| Sexual self-efficacy | 33.12 | 25 | 1.49 |
In addition, after removing the effect of the pretest, mindfulness-based cognitive therapy had a significant impact on conflict resolution (test coefficient [0, 24]: 5.69; P=0.025). Regarding the amount of confounding variable effect (i.e., mindfulness-based cognitive therapy), it can be said that (eta coefficient: 0.192) mindfulness-based cognitive therapy training was effective in the promotion of conflict resolution in the intervention group.
A repeated-measures ANOVA with a Greenhouse-Geisser correction determined that mean depression differed significantly between pretest, posttest, and follow-up phases (F=23.07; P<0.0005). Post hoc tests using the Bonferroni correction revealed that mindfulness-based cognitive therapy elicited a slight reduction in depression since pretraining to 3 months after training, which was statistically significant (P<0.001). However, posttraining marital satisfaction increased to 26.60±3.60, which was significantly different from that reported for the pretest (P<0.0005) and 3 months after the training therapy (P<0.001). Therefore, it can be concluded that a long-term mindfulness-based cognitive therapy program (i.e., 6 months) elicits a statistically significant increase in marital satisfaction.
The follow-up test showed that in mindfulness-based cognitive therapy, the mean of marital satisfaction at follow-up was not different from that of the posttest. Furthermore, the results of the follow-up test revealed that in the group receiving mindfulness-based cognitive therapy, the mean of sexual self-efficacy in the follow-up stage was not different from that of the posttest; nevertheless, the mean of sexual self-efficacy in the posttest stage was significantly higher than that reported for the pretest. In addition, the mean of sexual self-efficacy in the follow-up stage was significantly higher than that of the pretest (P<0.05). In the control group, there was no significant difference in different stages of the test (P<0.05).
Discussion
Mindfulness-based cognitive therapy affects the sexual self-efficacy of couples with marital conflicts. The findings of the present study showed that mindfulness-based cognitive therapy training has led to increased sexual self-efficacy in the intervention group. This result is in line with the findings of studies carried out by Burpee and Langer [21], Newcombe and Weaver [22], and Kanter et al. [23]. In explaining such a finding, it should be noted that mindfulness-based cognitive therapy helps to increase an individual’s ability to cope with difficult emotions, especially those associated with low sexual perception and self-concept.
In mindfulness-based cognitive therapy, the therapist wants the patient to postpone his/her judgment regarding his/her sexual experiences. Secondly, awareness is seriously concentrated on the events for some time. However, by the application of this technique, the patient experiences higher empowerment in his/her sexual relationships and will have higher self-efficacy [24]. In the confrontation technique of mindfulness-based cognitive therapy, the psychotherapist requires the patient to pay close attention to his or her sexual relationship and on the other hand impartially focus on his or her experiences, feelings, and perceptions. This attention leads to an increase in the perception of the positive aspects of sexual life and subsequently enhances sexual self-efficacy.
On the other hand, the therapist with cognitive change is trying to replace the pattern of maladaptive thinking about sexual incapability with sexual efficacy and empowerment. One of the critical points of mindfulness-based cognitive therapy is to emphasize that sexual self-efficacy is purely a subjective issue, and the interpretation that an individual considers him/herself weak regarding sexual relationship is truth or reality. On the other hand, during this course of treatment, the patient learns not to emotionally judge his/her sexual performance, stay calm, and thoroughly and impartially promote sexual self-efficacy by accepting and experiencing the sexual act [25].
In explaining such a finding, it should be noted that the mindfulness-based cognitive therapy training course empowers individuals to focus their attention on the experiences of emotions and events happening within themselves or around them at the moment. Through the introduction of metacognitive learning and new behavioral strategies, the therapist encourages the patient to pay more attention to his/her life issues and tries to reduce the rumination and inclination to worrying responses in the individual’s marital life. During the treatment, the patient is reminded that marital problems and differences are common in life, and the patient should respond to events with thought and reflection rather than responding involuntarily. In addition, the therapist teaches the patient to view the circumstances of his/her marital life and better know his/her emotions and accept them [25].
On the other hand, after undergoing mindfulness-based cognitive therapy, the patient can understand and digest physical phenomena and marital life events more easily and tries to use logical, rational, and consistent strategies in different situations of marital life; such a process leads to a coherent and sensible attitude toward the experiences of patient marital life and promotes marital satisfaction [26].
The mindfulness-based cognitive therapy course helps individuals modify negative behavioral patterns and automatic thoughts and adjust positive couple-friendly behaviors. In other words, mindfulness-based cognitive therapy through the combination of happiness and vivid view of marital life experiences can make positive changes in the patient’s mental states and increase the levels of marital satisfaction.
Undergoing mindfulness-based cognitive therapy allows the patient to use metacognitive and innovative behavioral strategies to focus on attention and prevent rumination and tendency to worry about responses. This ability in marital life enables the patient to spread his/her thoughts and effectively dispel unpleasant emotions from marital life. As a result, a patient with higher mindfulness due to having dominance at the right time and not fearing from life changes can create a consistently dynamic and flexible environment in his/her life [27, 28].
One of the limitations of the present study was a lack of the investigation of age, gender, and social groups (i.e., individuals of different ages, both genders, and different educational levels). Using a limited sample size of 15 individuals per group was another limitation of the current study. The short interval between the three stages of pretest, posttest, and follow-up was also another limitation of the current study. In addition, this study focused only on women with marital conflicts in Rasht, Iran, and the results should be cautiously generalized.
It is recommended to perform this therapy technique in future studies on other age groups, genders, psychological domains, and study groups by increasing the number of interventions and control groups to enhance the external validity and compare to other therapeutic outcomes. Using a higher number of participants in treatment courses can add to the validity of the research findings. The enrollment of different participants from other cities enhances the generalizability of the results.
Treatment courses with intervals can improve the effectiveness and durability of the results with greater validity. It is suggested to benefit from long-term efficacy courses in future studies. Given the impact of mindfulness-based cognitive therapy on sexual self-efficacy, it is recommended to offer such educational methods to therapists to use as therapeutic protocols in the domain of sexual problems.
Regarding the effect of mindfulness-based cognitive therapy on marital satisfaction, it is suggested to use the findings of the present study to design treatment courses and make decisions on family consolidation in counseling and family therapy centers. Considering the impact of mindfulness-based cognitive therapy on early maladaptive schemas, it is recommended to provide the proposed therapeutic model to welfare centers to empower the maladaptive unattended dysfunctional families.
Concerning the impact of mindfulness-based cognitive therapy on sexual self-efficacy, it is recommended to hold workshops for spouses to clarify the importance of this therapy and solve problems related to self-efficacy and sexual function. Considering the effect of mindfulness-based cognitive therapy on marital satisfaction, it is proposed to design possible implementation plans by health education centers and welfare organizations to provide the possibility of developing this program in family environments.
With regard to the effect of mindfulness-based cognitive therapy on early maladaptive schemas, it is suggested to increase the importance of this methodological approach in marital relationships by holding scientific conferences and seminars in this regard. In general, training and treatment programs can be run in counseling centers for married people or by performing specific workshops on mindfulness-based cognitive therapy and early maladaptive schemas to positively change the individual performance of couples.
Conclusions
Based on the obtained results, it can be concluded that mindfulness-based cognitive therapy can improve sexual self-efficacy and marital satisfaction in couples with marital conflicts.
Compliance with ethical guidelines
All the ethical principles were considered in the present study. The participants were informed about the purpose of the study and implementation of the stages. Furthermore, informed consent was obtained from all the study subjects. They were also assured of the confidentiality of their information. Moreover, the participants were allowed to withdraw from the study at any time, and the results of the study would be available to them if desired. The present study was extracted from a student’s doctoral thesis of health psychology approved by the Ethics Committee of Islamic Azad University of Rasht with the ethics code of IR.IAURASHT.REC.1397.012.
Acknowledgments
The authors would like to express their gratitude to the participants, who greatly cooperated with this study.
Funding/Support
The current study did not receive any specific grant from funding agencies in public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declare that there is no conflict of interest.
References
A repeated-measures ANOVA with a Greenhouse-Geisser correction determined that mean depression differed significantly between pretest, posttest, and follow-up phases (F=23.07; P<0.0005). Post hoc tests using the Bonferroni correction revealed that mindfulness-based cognitive therapy elicited a slight reduction in depression since pretraining to 3 months after training, which was statistically significant (P<0.001). However, posttraining marital satisfaction increased to 26.60±3.60, which was significantly different from that reported for the pretest (P<0.0005) and 3 months after the training therapy (P<0.001). Therefore, it can be concluded that a long-term mindfulness-based cognitive therapy program (i.e., 6 months) elicits a statistically significant increase in marital satisfaction.
The follow-up test showed that in mindfulness-based cognitive therapy, the mean of marital satisfaction at follow-up was not different from that of the posttest. Furthermore, the results of the follow-up test revealed that in the group receiving mindfulness-based cognitive therapy, the mean of sexual self-efficacy in the follow-up stage was not different from that of the posttest; nevertheless, the mean of sexual self-efficacy in the posttest stage was significantly higher than that reported for the pretest. In addition, the mean of sexual self-efficacy in the follow-up stage was significantly higher than that of the pretest (P<0.05). In the control group, there was no significant difference in different stages of the test (P<0.05).
Discussion
Mindfulness-based cognitive therapy affects the sexual self-efficacy of couples with marital conflicts. The findings of the present study showed that mindfulness-based cognitive therapy training has led to increased sexual self-efficacy in the intervention group. This result is in line with the findings of studies carried out by Burpee and Langer [21], Newcombe and Weaver [22], and Kanter et al. [23]. In explaining such a finding, it should be noted that mindfulness-based cognitive therapy helps to increase an individual’s ability to cope with difficult emotions, especially those associated with low sexual perception and self-concept.
In mindfulness-based cognitive therapy, the therapist wants the patient to postpone his/her judgment regarding his/her sexual experiences. Secondly, awareness is seriously concentrated on the events for some time. However, by the application of this technique, the patient experiences higher empowerment in his/her sexual relationships and will have higher self-efficacy [24]. In the confrontation technique of mindfulness-based cognitive therapy, the psychotherapist requires the patient to pay close attention to his or her sexual relationship and on the other hand impartially focus on his or her experiences, feelings, and perceptions. This attention leads to an increase in the perception of the positive aspects of sexual life and subsequently enhances sexual self-efficacy.
On the other hand, the therapist with cognitive change is trying to replace the pattern of maladaptive thinking about sexual incapability with sexual efficacy and empowerment. One of the critical points of mindfulness-based cognitive therapy is to emphasize that sexual self-efficacy is purely a subjective issue, and the interpretation that an individual considers him/herself weak regarding sexual relationship is truth or reality. On the other hand, during this course of treatment, the patient learns not to emotionally judge his/her sexual performance, stay calm, and thoroughly and impartially promote sexual self-efficacy by accepting and experiencing the sexual act [25].
In explaining such a finding, it should be noted that the mindfulness-based cognitive therapy training course empowers individuals to focus their attention on the experiences of emotions and events happening within themselves or around them at the moment. Through the introduction of metacognitive learning and new behavioral strategies, the therapist encourages the patient to pay more attention to his/her life issues and tries to reduce the rumination and inclination to worrying responses in the individual’s marital life. During the treatment, the patient is reminded that marital problems and differences are common in life, and the patient should respond to events with thought and reflection rather than responding involuntarily. In addition, the therapist teaches the patient to view the circumstances of his/her marital life and better know his/her emotions and accept them [25].
On the other hand, after undergoing mindfulness-based cognitive therapy, the patient can understand and digest physical phenomena and marital life events more easily and tries to use logical, rational, and consistent strategies in different situations of marital life; such a process leads to a coherent and sensible attitude toward the experiences of patient marital life and promotes marital satisfaction [26].
The mindfulness-based cognitive therapy course helps individuals modify negative behavioral patterns and automatic thoughts and adjust positive couple-friendly behaviors. In other words, mindfulness-based cognitive therapy through the combination of happiness and vivid view of marital life experiences can make positive changes in the patient’s mental states and increase the levels of marital satisfaction.
Undergoing mindfulness-based cognitive therapy allows the patient to use metacognitive and innovative behavioral strategies to focus on attention and prevent rumination and tendency to worry about responses. This ability in marital life enables the patient to spread his/her thoughts and effectively dispel unpleasant emotions from marital life. As a result, a patient with higher mindfulness due to having dominance at the right time and not fearing from life changes can create a consistently dynamic and flexible environment in his/her life [27, 28].
One of the limitations of the present study was a lack of the investigation of age, gender, and social groups (i.e., individuals of different ages, both genders, and different educational levels). Using a limited sample size of 15 individuals per group was another limitation of the current study. The short interval between the three stages of pretest, posttest, and follow-up was also another limitation of the current study. In addition, this study focused only on women with marital conflicts in Rasht, Iran, and the results should be cautiously generalized.
It is recommended to perform this therapy technique in future studies on other age groups, genders, psychological domains, and study groups by increasing the number of interventions and control groups to enhance the external validity and compare to other therapeutic outcomes. Using a higher number of participants in treatment courses can add to the validity of the research findings. The enrollment of different participants from other cities enhances the generalizability of the results.
Treatment courses with intervals can improve the effectiveness and durability of the results with greater validity. It is suggested to benefit from long-term efficacy courses in future studies. Given the impact of mindfulness-based cognitive therapy on sexual self-efficacy, it is recommended to offer such educational methods to therapists to use as therapeutic protocols in the domain of sexual problems.
Regarding the effect of mindfulness-based cognitive therapy on marital satisfaction, it is suggested to use the findings of the present study to design treatment courses and make decisions on family consolidation in counseling and family therapy centers. Considering the impact of mindfulness-based cognitive therapy on early maladaptive schemas, it is recommended to provide the proposed therapeutic model to welfare centers to empower the maladaptive unattended dysfunctional families.
Concerning the impact of mindfulness-based cognitive therapy on sexual self-efficacy, it is recommended to hold workshops for spouses to clarify the importance of this therapy and solve problems related to self-efficacy and sexual function. Considering the effect of mindfulness-based cognitive therapy on marital satisfaction, it is proposed to design possible implementation plans by health education centers and welfare organizations to provide the possibility of developing this program in family environments.
With regard to the effect of mindfulness-based cognitive therapy on early maladaptive schemas, it is suggested to increase the importance of this methodological approach in marital relationships by holding scientific conferences and seminars in this regard. In general, training and treatment programs can be run in counseling centers for married people or by performing specific workshops on mindfulness-based cognitive therapy and early maladaptive schemas to positively change the individual performance of couples.
Conclusions
Based on the obtained results, it can be concluded that mindfulness-based cognitive therapy can improve sexual self-efficacy and marital satisfaction in couples with marital conflicts.
Compliance with ethical guidelines
All the ethical principles were considered in the present study. The participants were informed about the purpose of the study and implementation of the stages. Furthermore, informed consent was obtained from all the study subjects. They were also assured of the confidentiality of their information. Moreover, the participants were allowed to withdraw from the study at any time, and the results of the study would be available to them if desired. The present study was extracted from a student’s doctoral thesis of health psychology approved by the Ethics Committee of Islamic Azad University of Rasht with the ethics code of IR.IAURASHT.REC.1397.012.
Acknowledgments
The authors would like to express their gratitude to the participants, who greatly cooperated with this study.
Funding/Support
The current study did not receive any specific grant from funding agencies in public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declare that there is no conflict of interest.
References
- Montesi JL, Fauber RL, Gordon EA, Heimberg RG. The specific importance of communicating about sex to couples' sexual and overall relationship satisfaction. Journal of Social and Personal Relationships. 2011; 28(5):591-609. [DOI:10.1177/0265407510386833]
- Heiman JR, Long JS, Smith SN, Fisher WA, Sand MS, Rosen RC. Sexual satisfaction and relationship happiness in midlife and older couples in five countries. Archives of Sexual Behavior. 2011; 40(4):741-53. [DOI:10.1007/s10508-010-9703-3] [PMID]
- Dosch A, Rochat L, Ghisletta P, Favez N, Van der Linden M. Psychological factors involved in sexual desire, sexual activity, and sexual satisfaction: a multi-factorial perspective. Archives of Sexual Behavior. 2016; 45(8)1-17. [DOI:10.1007/s10508-014-0467-z] [PMID]
- Yeh HC, Lorenz F, Wickrama KA, Conger RD, Elder G Jr. Relationships among sexual satisfaction, marital quality, and marital instability at midlife. Journal of Family Psychology. 2006; 20(2):339-43. [DOI:10.1037/0893-3200.20.2.339] [PMID]
- del Mar Sánchez-Fuentes M, Santos-Iglesias P, Sierra JC. A systematic review of sexual satisfaction. International Journal of Clinical and Health Psychology. 2014; 14(1):67-75. [DOI:10.1016/S1697-2600(14)70038-9]
- Thomas H, Hess R, Thurston R. Correlates of sexual activity and satisfaction in midlife and older women. Annals of Family Medicine. 2015; 13(4):336-42. [DOI:10.1370/afm.
1820] [PMID] [PMCID] - MacNeil S, Byers ES. Role of sexual self-disclosure in the sexual satisfaction of long-term heterosexual couples. Journal of Sex Research. 2009; 46(1):3-14. [DOI:10.1080/
00224490802398399] [PMID] - Simonelli C, Eleuteri S, Petruccelli F, Rossi R. Female sexual pain disorders: dyspareunia and vaginismus. Current Opinion in Psychiatry. 2014; 27(6):406-12. [DOI:10.1097/
YCO.0000000000000098] [PMID] - Rosenbaum TY. An integrated mindfulness-based approach to the treatment of women with sexual pain and anxiety: promoting autonomy and mind/body connection. Sexual and Relationship Therapy. 2013; 28(1-2):20-8. [DOI:10.
1080/14681994.2013.764981] - Brotto LA, Basson R, Smith KB, Driscoll M, Sadownik L. Mindfulness-based group therapy for women with provoked vestibulodynia. Mindfulness. 2015; 6(3):417-32. [DOI:10.
1007/s12671-013-0273-z] - Dunkley CR, Brotto LA. Psychological treatments for provoked vestibulodynia: integration of mindfulness‐based and cognitive behavioral therapies. Journal of Clinical Psychology. 2016; 72(7):637-50. [DOI:10.1002/jclp.22286] [PMID]
- Bayles C. Using mindfulness in a harm reduction approach to substance abuse treatment: a literature review. International Journal of Behavioral Consultation and Therapy. 2014; 9(2):22. [DOI:10.1037/h0100995]
- Lazaridou A, Kalogianni C. Mindfulness and sexuality. Sexual and Relationship Therapy. 2013; 28(1-2):29-38. [DOI:10.1080/14681994.2013.773398]
- Kimbrough E, Magyari T, Langenberg P, Chesney M, Berman B. Mindfulness intervention for child abuse survivors. Journal of Clinical Psychology. 2010; 66(1):17-33. [DOI:10.1002/jclp.20624] [PMID]
- Mize SJ. A review of mindfulness-based sex therapy interventions for sexual desire and arousal difficulties: from research to practice. Current Sexual Health Reports. 2015; 7(2):89-97. [DOI:10.1007/s11930-015-0048-8]
- Byrne J, Hauck Y, Fisher C, Bayes S, Schutze R. Effectiveness of a mindfulness‐based childbirth education pilot study on maternal self‐efficacy and fear of childbirth. Journal of Midwifery & Women's Health. 2014; 59(2):192-7. [DOI:10.1111/jmwh.12075] [PMID]
- Nooripour R, Bass CK, Apsche J. Effectiveness of quality of life therapy aimed at improving sexual self-efficacy and marital satisfaction in addict couples of treatment period. International Journal of Behavioral Consultation and Therapy. 2013; 8(2):26. [DOI:10.1037/h0100973]
- Price CJ, Wells EA, Donovan DM, Rue T. Mindful awareness in body-oriented therapy as an adjunct to women's substance use disorder treatment: a pilot feasibility study. Journal of Substance Abuse Treatment. 2012; 43(1):94-107. [DOI:10.1016/j.jsat.2011.09.016] [PMID] [PMCID]
- Farnam F, Pakgohar M, Mir-mohammadali M. Effect of pre-marriage counseling on marital satisfaction of Iranian newlywed couples: a randomized controlled trial. Sexuality & Culture. 2011; 15(2):141-52. [DOI:10.1007/s12119-010-9086-6]
- Askari M, B Mohd Noah S, Aishah Bt Hassan S, Bt Baba M. Comparison the effects of communication and conflict resolution skills training on marital satisfaction. International Journal of Psychological Studies. 2013; 5(1):91-104. [DOI:10.5539/ijps.v5n1p91]
- Burpee LC, Langer EJ. Mindfulness and marital satisfaction. Journal of Adult Development. 2005; 12(1):43-51. [DOI:10.1007/s10804-005-1281-6]
- Newcombe BC, Weaver AD. Mindfulness, cognitive distraction, and sexual well-being in women. The Canadian Journal of Human Sexuality. 2016; 25(2):99-108. [DOI:10.3138/cjhs.252-A3]
- Kanter G, Komesu YM, Qaedan F, Jeppson PC, Dunivan GC, Cichowski SB, et al. Mindfulness-based stress reduction as a novel treatment for interstitial cystitis/bladder pain syndrome: a randomized controlled trial. International Urogynecology Journal. 2016; 27(11):1705-11. [DOI:10.
1007/s00192-016-3022-8] [PMID] [PMCID] - Kimmes JG, Mallory AB, Cameron C, Köse Ö. A treatment model for anxiety-related sexual dysfunctions using mindfulness meditation within a sex-positive framework. Sexual and Relationship Therapy. 2015; 30(2):286-96. [DOI:10.1080/14681994.2015.1013023]
- Stephenson KR. Mindfulness-based therapies for sexual dysfunction: a review of potential theory-based mechanisms of change. Mindfulness. 2017; 8(3):527-43. [DOI:10.
1007/s12671-016-0652-3] - Gambrel LE, Keeling ML. Relational aspects of mindfulness: implications for the practice of marriage and family therapy. Contemporary Family Therapy. 2010; 32(4):412-26. [DOI:10.1007/s10591-010-9129-z]
- Zainal NZ, Booth S, Huppert FA. The efficacy of mindfulness‐based stress reduction on mental health of breast cancer patients: a meta‐analysis. Psychooncology. 2013; 22(7):1457-65. [DOI:10.1002/pon.3171] [PMID]
- Bossio JA, Basson R, Driscoll M, Correia S, Brotto LA. Mindfulness-based group therapy for men with situational erectile dysfunction: a mixed-methods feasibility analysis and pilot study. The Journal of Sexual Medicine. 2018; 15(10):1478-90. [DOI:10.1016/j.jsxm.2018.08.013] [PMID]
Article Type: Research Article |
Subject:
Sexual behavior
Received: 2020/08/12 | Accepted: 2020/08/20 | Published: 2020/08/20
Received: 2020/08/12 | Accepted: 2020/08/20 | Published: 2020/08/20
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Hamadan University of Medical Sciences.
Published by UMSHA Press
Journal Tel: +989025126654
Publisher Tel: +985138419434
Website: http://ajnpp.umsha.ac.ir
Email: avicennajnpp[at]gmail.com
