




BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://ajnpp.umsha.ac.ir/article-1-188-en.html



2- Department of Psychology, Islamic Azad University, Karaj Branch, Karaj, Iran. , btajeri@yahoo.com
3- Department of Psychology, Islamic Azad University, Karaj Branch, Karaj, Iran.
4- Department of Psychology, Allameh Tabatabayi, Tehran, Iran.
Introduction
Due to the nature of the disease and its long-term complications, diabetes is classified as a chronic disorder that has no definitive medication; however, it is manageable. Implementation and continuation of self-care behaviors by the patient, together with family participation, can prevent or delay the acute and chronic complications of the disease [1]. This is of concern because type 2 diabetes is one of the largest public health problems facing the United States today, affecting approximately 8% of the US population [2]. Diabetic patient’s adherence to the drug regimen 76% and 65.86%, respectively [3]. One of the essential goals of educating the patients is to encourage them to pursue medication and improve their quality of life [4].
Adherence to treatment is effective in preventing illness and life expectancy. While facing health problems, people are less likely to seek medication, which can be a consequence of the severity and chronicity of the medication [5]. These adherence behaviors include adherence to medications that control hyperglycemia and the metabolic conditions associated with type 2 diabetes, such as hypertension and hyperlipidemia, adherence to dietary recommendations aimed at lowering blood glucose by reducing body weight and improving diet composition, increasing physical activity to improve insulin sensitivity and facilitate weight loss, self-monitoring of blood glucose levels to measure fluctuations in glucose and the impact of behavioral factors on glucose levels (e.g. medication, exercise, and diet), and proper preventive foot care to reduce the risk of podiatric complications [6].
Generally, diabetics like patients with other chronic illnesses exhibit suboptimal adherence to medical recommendations, with patients with diabetes exhibiting the second-lowest adherence rate compared with 17 chronic illnesses [7]. Misconceptions about diabetes and its treatment are prevalent and associated with worse diabetes control [8], and also concerns about the negative effects of treatment, which are often unfounded, are associated with nonadherence to antihyperglycemic and antihypertensive treatments and worsen diabetes and hypertension control in patients with diabetes [9]. Thus, cognitive dysfunction has been identified as one of the predictors of non-medication adherence among diabetic patients. Patients’ cognitive processes and perceptions are two essential factors that indirectly affect satisfaction with medication and also directly affect compliance. Psychological interventions based on cognitive-behavioral principles were significantly helpful in the psychological states of diabetic patients [10].
Cognitive-Behavioral Therapy for Adherence and Depression (CBT-AD) was originally developed for patients with HIV that integrates CBT for depression with a CBT intervention designed to promote medication adherence. In the first session of CBT, beliefs about illness and treatment are elicited from patients, and special attention is paid to the cognitions related to the specific treatment regimen of each patient. Subsequently, cognitive restructuring techniques are employed to challenge maladaptive cognitions. Behavioral strategies and problem-solving approaches are also employed to support successful adherence [11]. CBT has been successful in improving adherence in a randomized controlled trial of patients with depression and HIV, in which the full intervention was compared with a brief intervention focusing on adherence alone [12]. Additionally, Mohr et al. [11] indicated that CBT improved adherence compared with face-to-face delivery; however, the increased risk of poorer maintenance of gains was observed after treatment cessation.
Promoting public health requires training in healthy lifestyles, adaptive coping behaviors, and helping at-risk people. People with a set of coping skills and abilities are more likely to face problems. Using effective coping strategies helps them overcome physical and psychological problems, interpersonal and social relationships, and personal conflicts [13]. Therefore, they have a better quality of life and mental health. In contrast, people who use emotional or avoidance strategies are more likely to be exposed to emotional and attitude burnout [14]. The theory of conservation motivation includes threat assessment and evaluation of coping and fear constructs that lead to protection and behavior motivation. The threat assessment includes perceived susceptibility, perceived severity, and perceived rewards (perceived internal and external rewards), and coping assessment includes perceived self-efficacy, perceived response efficacy, and perceived response costs. Fear is an intermediate variable between perceived sensitivity and threat assessment [15]. According to various studies, the constructs of this theory are capable of predicting different protective behaviors, such as cancer prevention, smoking cessation, and physical activity [15, 16].
Unlike HIV self-management, which primarily consists of medication adherence, diabetes self-care is composed of several additional important adherence behaviors necessary to control disease progress (e.g. glucose monitoring, diet, exercise, and foot care), that requires adaptation of the original intervention. The present study was designed to compare the effectiveness of CBT and education based on protection motivation adherence to treatment in patients with diabetes.
Materials and Methods
The present quasi-experimental study with the pre-test-post-test, a control group, and follow-up was conducted on all women aged 40-65 years with diabetes who referred to the Diabetes Association of Tehran. Using the convenience sampling method, almost 45 patients were selected through advertisements and posters from the patients of the Tehran Diabetes Association and those referring to the health-related clinics. The subjects were randomly assigned to three groups: Two experimental and one control groups (n=15 per group). Inclusion criteria for the experimental groups included using no psychotropic medications and other substances during the study, the age of over 40 years, and no acute or chronic mental disorders. The exclusion criteria for the experimental groups included loss of the trial and intervention for more than two sessions, unwillingness to continue the intervention, severe psychiatric disorder requiring urgent medication, and using psychotropic drugs or substances.
The ethical consideration in this research was as follows: Before starting and participating in the research, the subjects were informed about the research objectives. The attitudes and beliefs of the individuals were respected. The members of the experimental and control groups were allowed to leave the research project at any stage. Also, the control group members were free to repeat the treatment sessions of the experimental group, if desired only at the end of the treatment. All documents and questionnaires and confidential records were only available to the administrators. A written and informed consent was taken from the parents or legal protectors of all the candidates.
Morisky Medication Adherence Scale
Medication Adherence Scale is a self-report questionnaire designed in 2010 by Morisky et al. In this scale, the high medication adherence is scored 8 out of 8, average medication 6 out of 8, and low medication adherence is lower than 6. This scale is a previously validated 4-item scale that was developed and supplemented with other items including conditions that need receiving medication [17]. Its reliability using the Cronbach’s alpha coefficient was 0.89, which indicates the optimal reliability of this scale [18].
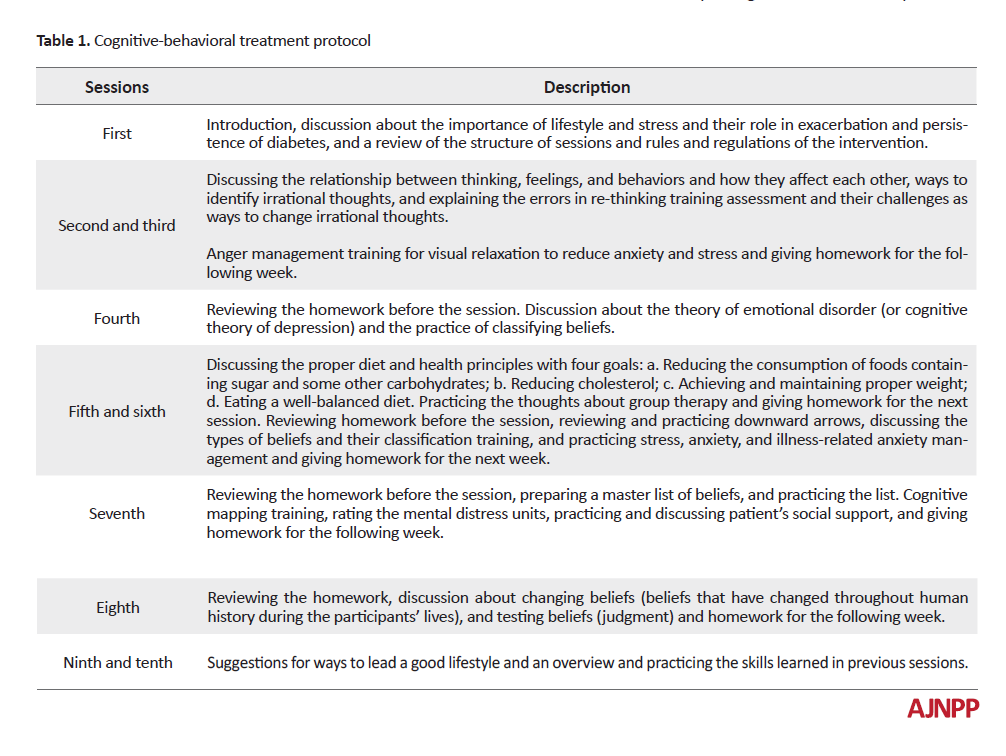
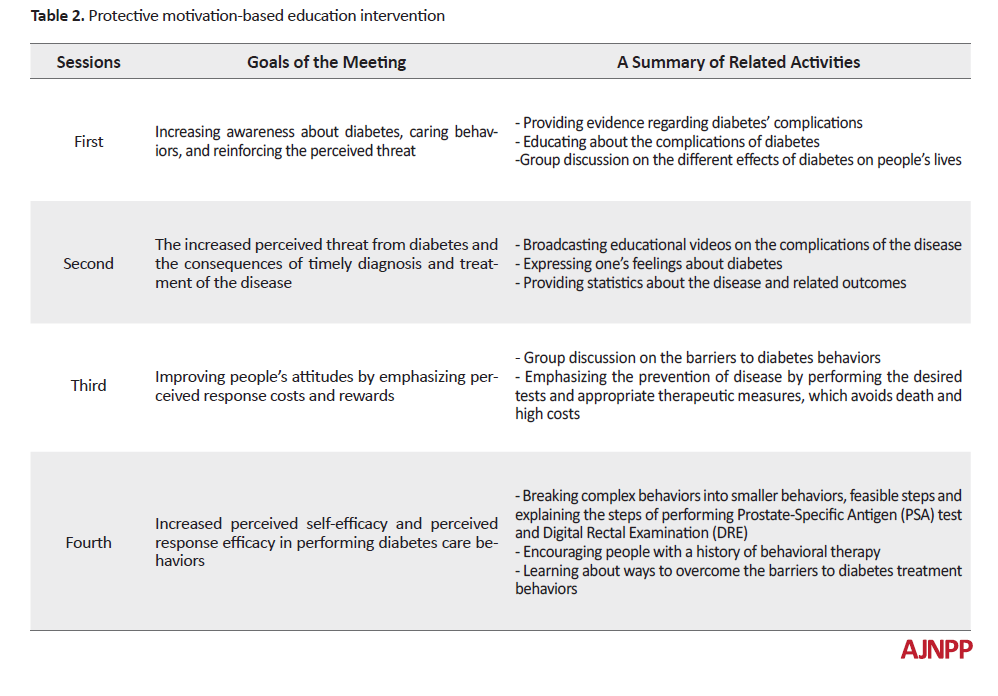
After obtaining research approval from the Diabetes Association of Tehran and setting the research goals, the Medication Adherence Scale and a personal information form were provided to the experimental and control groups to collect data. To perform these interventions, therapeutic sessions were held for 90 min once a week at the Diabetes Association. Before the treatment sessions, a briefing session of 45 min was held separately for the experimental and control group members. Each CBT session for the first experimental group began with relaxation training, including relaxation techniques. In the second part of each session, cognitive-behavioral techniques associated with patients’ health issues were taught. After three months of treatment, the subjects were re-tested to see whether the treatment was effective and to what extent. Also, the second experimental group received a protective motivation-based training intervention, and a 90-day follow-up was considered for this group. The medication plan was implemented based on a CBT and a structured approach (Table 1 & 2).
Repeated measures ANOVA and analysis of covariance (ANCOVA) were used to analyze the data, and the Bonferroni test was used to compare the results of the experimental and control groups by SPSS V. 22.
Results
The subjects included 45 women with the age range of 40-65 years. Regarding education, 4 cases (8%) had an undergraduate degree, 29 cases (64%) had a bachelor’s degree, 8 subjects (17%) had a master’s degree, and 4 cases (8%) had PhD. The higher Cronbach’s alpha values indicated the high validity of the research questionnaire. A mixed analysis of variance was used for statistical analysis. In this hypothesis, the group factor with three levels of CBT, motivational-based education and control, and the time factor with three levels of pre-test, post-test, and follow-up were evaluated. Before performing the analysis of variance, its assumptions, i.e. normal distribution of data and homogeneity of variances and linear slopes were first examined. Kolmogorov-Smirnov test was used to test the normal distribution of data.
Given that the significance level was higher than 0.05, it was concluded that the distribution of data in the three groups was normal. Also, the variances of the two groups were equal and homogeneous. Therefore, the assumption of homogeneity of variances for this variable was fulfilled. The significant level of interaction between the two groups was higher than 0.01; therefore, the calculated F and the interaction were not statistically significant and the assumption of homogeneity of the regression slopes was confirmed. After checking the normal distribution of data, the assumptions of homogeneity of variance, the equality of variance, and homogeneity of linear slopes, the researcher could use the analysis of variance.
The results of Table 3 showed that adherence to treatment in the pre-test of the CBT group increased from 5.11 (2.1) to 7.56 (2.2) in the post-test (P<0.001).

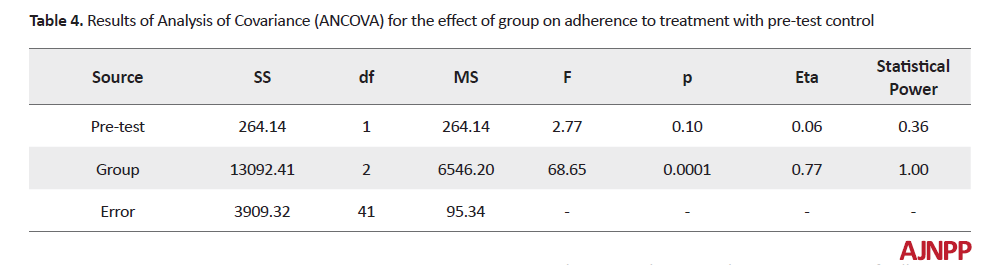
Also, adherence to treatment in the pre-test in the motivation group increased from 5.03 (1.5) to 6.98 (1.9) in the post-test (P<0.01); however, there was no significant difference between the control group in terms of adherence to treatment in pre-test and post-test (P>0.05) (Table 4).
Mauchly’s Test of Sphericity indicated that the assumption of sphericity was violated, (χ2=22.115, P<0.0005); therefore, a Greenhouse-Geisser correction was used. According to the results, the effect of time on adherence to treatment was found significant (F(1.171, 38)0=021.032, P<0.0005).
According to the findings in Table 5, the effects of CBT and motivation-based training were significant in reducing post-test and follow-up scores (F(2,42)=43.50, P<0.0001).

The effect of the time on follow-up scores at the follow-up stage was also significant (F=124.22, P<0.001). Therefore, it can be concluded that there was a difference between the adherence to treatment scores in three stages of pre-test, post-test, and follow-up regardless of group. The effect of interaction between group and time was also significant (F=36.20, P<0.001). Therefore, the group effect was different concerning the time point of measurement. Also, considering the Chi-square value of 0.23, it can be concluded that the intervention resulted in changes in the experimental group and the medication intervention was effective in adherence to treatment. Then, to investigate the effect of interaction between group and time on treatment scores (time was considered constant), the mean of adherence to treatment in groups at each measurement stage was compared using the Bonferroni post-hoc test.
The results of Table 6 indicated a significant difference between the mean of post-test and pre-test scores regarding adherence to treatment.

Also, there was a statistically significant difference between the mean scores of the two experimental and control groups. Therefore, it can be concluded that the CBT and protective motivation-based training groups indicated a significant increase in adherence to treatment compared with the control group. CBT was more effective than motivation-based education in adherence to treatment in the post-test and follow-up and can be used to improve adherence to treatment in patients with type 2 diabetes.
Discussion
The findings of this study indicated that the effectiveness of CBT and motivation-based education in adherence to treatment among patients with type 2 diabetes is different. CBT was more effective than motivation-based education in adherence to treatment in the post-test and follow-up stages. The findings of this study are consistent with the results reported in previous studies [11, 12]. Many factors play a key role in patients' medication treatment, of which the patient and prescriber-related factors are the most important. The effectiveness of increasing the education of the patients and physicians by providing educational pamphlets to increase the patient’s adherence to treatment was shown in numerous studies [19].
No study was found comparing the efficacy of these two training programs in the process of following and controlling diabetes in patients with diabetes. CBT was also found effective in increasing medication adherence, improving stress management, and controlling disease among diabetic patients [9]. In this regard, Kaplan believes that motivated individuals are more involved in health-promoting behaviors and daily activities and also they enjoy challenges and prefer them rather than stability [20]. These people can identify stress levels and take various measures to reduce the impact of stress on their lives. They have a good view of stress and classify stresses and respond to them according to their severity. Therefore, they can maintain their strength under stressful conditions and face problem-solving coping skills reasonably with their disease issues [21]. Therefore, they are less likely to be affected by destructive social relationships and use social communication to improve their lives. Nowadays, medication adherence and adherence to medical advice are some of the critical concerns of the medical team. Researchers believe the lack of adherence to the recommendations of the experts can put at the patients at a higher risk of complications and non-adherence can have dangerous consequences for them [22]. Also, the lack of motivation to change the behavior, as well as the long-term use of prescribed drugs are the essential factors that can lead to failure of treatment in these patients. The vital principles of adherence, participation, and acceptance of responsibility are the patient’s responsibilities [23].
Training to protect diabetic patients changes this interactive relationship for the benefit of the patient and in a positive direction [24]. Moreover, the body’s metabolism system is unbalanced in response to fear and this causes the blood sugar level to be disturbed, and consequently, the patient's prescription drug dosage is inconsistent. Because the adrenaline, noradrenaline, and other stress hormones secretion increases from the adrenal glands in response to fear, and because of the effect of these hormones on the liver, the formulation of converting hepatic reserves into glucose (sugar) to supply the energy needed for the fight-and-flight response process is disturbed leading to increased blood sugar [25]. Therefore, the protection motivation training for diabetic patients can reduce and control their blood sugar by helping patients to cope with the fear of anxiety and reducing the frequency and intensity of fear experiences. Besides, applying fear management techniques in daily life and receiving positive feedback from it increases the effectiveness of diabetic patients and increases their anxiety in disease management.
On the other hand, by examining the content of the presentations in CBT sessions in this study, using cognitive strategies, such as problem recognition, cognitive errors, combating negative thoughts, rational thinking, and the use of positive self-talk may change the attitudes and cognitions of affected patients, so that the patients can accept their disease and face its psychological consequences more reasonably and took steps to improve themselves and control their disease more effectively using the learned skills. Having such an ability plays a vital role in providing mental health because worrying about the disease and its consequences and negative attitude to treatment leads to taking a great deal of mental energy and can be a source of fear, frustration, and a sense of failure in many cases. Also, the vigilance and waiting for occurring symptoms and complications reduced in patients to some extent in this training through controlling automatic negative thoughts and helping patients manage the effects of the disease in their minds. They also could manage and control their fear and anxiety, which makes them feel more relaxed and more effectively controlled [10]. In general, the efficacy of CBT in adherence to treatment among patients with type 2 diabetes can be explained by factors, such as recognizing the disease and adjusting to its current situation, patients' positive expectations about the future, and learning how to deal effectively.
One of the features of CBT is increasing awareness and enhancing skills, which is important in its effectiveness in comparison with protective motivation intervention. As the limitations of the research, the sample was limited to the available cases and also we faced the time limit; therefore, studying in a more extended period (test and follow-up) can result in more accurate outcomes regarding the interventions. Also, this study did not provide an opportunity due to administrative, financial, and time constraints. In this regard, it is recommended that educational packages be tailored to the different groups based on the latest scientific methods to improve adherence to treatment and quality of life for these individuals, as well as at the community level. It is recommended to design a specific program by specialists for diabetic patients, and the formal integration of this training into diabetes care-care programs be considered by the supervisors and institutions expert in the field.
Conclusion
It can be concluded that CBT and motivation-based education could improve adherence to treatment in patients with type 2 diabetes. CBT was more effective than motivation-based education in adherence to treatment in post-test and follow-up stages and can be used to improve adherence to treatment in patients with type 2 diabetes.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages and signed the informed consent. They were also assured of the confidentiality of their information. Moreover, they were allowed to leave the study whenever they wish, and if desired, and the results of the research would be available to them. This article was extracted from a Ph.D. dissertation in Health Psychology of the Islamic Azad University, Emirates Branch, and approved by the Ethics Committee of this University (Code: IR.IAU.AE.REC.1398.12).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally in preparing all parts of the research.
Conflict of interest
The authors declared no conflict of interests.
References
1.Hernandez-Tejada MA, Campbell JA, Walker RJ, Smalls BL, Davis KS, Egede LE. Diabetes empowerment, medication adherence, and self-care behaviors in adults with type 2 diabetes. Diabetes Technology & Therapeutics. 2012; 14(7):630-4. [DOI:10.1089/dia.2011.0287] [PMID] [PMCID]
2.Esposito K, Maiorino MI, Bellastella G, Panagiotakos DB, Giugliano D. Mediterranean diet for type 2 diabetes: Cardiometabolic benefits. Endocrine. 2017; 56(1):27-32. [DOI:10.1007/s12020-016-1018-2] [PMID]
3.Esteghamati A, Gouya MM, Abbasi M, Delavari A, Alikhani S, Alaedini F, et al. Prevalence of diabetes and impaired fasting glucose in the adult population of Iran: National Survey of Risk Factors for Non-Communicable Diseases of Iran. Diabetes Care. 2008; 31(1):96-8. [DOI:10.2337/dc07-0959] [PMID]
4.Figueira ALG, Boas LCGV, Coelho ACM, Freitas MCF de, Pace AE. Educational interventions for knowledge on the disease, treatment adherence and control of diabetes mellitus. Revista Latino-Americana de Enfermagem. 2017; 25:e2863. [DOI:10.1590/1518-8345.1648.2863] [PMID] [PMCID]
5.Shao Y, Liang L, Shi L, Wan C, Yu S. The effect of social support on glycemic control in patients with type 2 diabetes mellitus: The mediating roles of self-efficacy and adherence. Journal of Diabetes Research. 2017; 2017:2804178. [DOI:10.1155/2017/2804178] [PMID] [PMCID]
6.Parajuli J, Saleh F, Thapa N, Ali L. Factors associated with nonadherence to diet and physical activity among Nepalese type 2 diabetes patients: A cross sectional study. BMC Research Notes. 2014; 7(1):758. [DOI:10.1186/1756-0500-7-758] [PMID] [PMCID]
7.Rwegerera GM. Adherence to anti-diabetic drugs among patients with type 2 diabetes mellitus at Muhimbili National Hospital, Dar es Salaam, Tanzania: A cross-sectional study. The Pan African Medical Journal. 2014; 17. [DOI:10.11604/pamj.2014.17.252.2972] [PMCID]
8.Connelly J, Kirk A, Masthoff J, MacRury S. The use of technology to promote physical activity in type 2 diabetes management: A systematic review. Diabetic Medicine. 2013; 30(12):1420-32. [DOI:10.1111/dme.12289] [PMID]
9.Noser AE, Huffhines L, Clements MA, Patton SR. Diabetes conflict outstrips the positive impact of self-efficacy on youth adherence and glycemic control in type 1 diabetes. Pediatric Diabetes. 2017; 18(7):614-8. [DOI:10.1111/pedi.12471] [PMID] [PMCID]
10.Safren SA, O’Cleirigh CM, Bullis JR, Otto MW, Stein MD, Pollack MH. Cognitive behavioral therapy for adherence and depression (CBT-AD) in HIV-infected injection drug users: A randomized controlled trial. Journal of Consulting and Clinical Psychology. 2012; 80(3):404. [DOI:10.1037/a0028208] [PMID] [PMCID]
11.Mohr DC, Ho J, Duffecy J, Reifler D, Sokol L, Burns MN, et al. Effect of telephone-administered vs face-to-face cognitive behavioral therapy on adherence to therapy and depression outcomes among primary care patients: A randomized trial. JAMA. 2012; 307(21):2278-85. [DOI:10.1001/jama.2012.5588] [PMID] [PMCID]
12.Safren SA, O’Cleirigh C, Tan JY, Raminani SR, Reilly LC, Otto MW, et al. A randomized controlled trial of Cognitive Behavioral Therapy for Adherence and Depression (CBT-AD) in HIV-infected individuals. Health Psychology. 2009; 28(1):1-10. [DOI:10.1037/a0012715] [PMID] [PMCID]
13.Mirkarimi K, Charkazi AR, Honarvar MR, Kabir MJ, Berdi Ozouni-Davaji R, Aryaie M, et al. Effect of motivational interviewing on physical activity intention among obese and overweight women using protection motivation theory: A randomized clinical trial. The Horizon of Medical Sciences. 2016; 22(4):321-7. [DOI:10.18869/acadpub.hms.22.4.321]
14.Rahaei Z, Ghofranipour F, Morowatisharifabad MA, Mohammadi E. Determinants of cancer early detection behaviors: Application of protection motivation theory. Health Promotion Perspectives. 2015; 5(2):138-46. [DOI:10.15171/hpp.2015.016] [PMID] [PMCID]
15.Yan Y, Jacques-Tiura AJ, Chen X, Xie N, Chen J, Yang N, et al. Application of the protection motivation theory in predicting cigarette smoking among adolescents in China. Addictive Behaviors. 2014; 39(1):181-8. [DOI:10.1016/j.addbeh.2013.09.027] [PMID] [PMCID]
16.Tazval J, Ghafari M, Mohtashami Yeganeh F, Babazadeh T, Rabati R. Efficiency of protection motivation theory on prediction of skin cancer and sunlight preventive behaviors in farmers in Ilam county. Journal of Health. 2017;7(5):656-67. [http://healthjournal.arums.ac.ir/article-1-1096-en.html.]
17.Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. Journal of Clinical Hypertension (Greenwich, Conn.). 2008; 10(5):348-54. [DOI:10.1111/j.1751-7176.2008.07572.x] [PMID] [PMCID]
18.Tomaszewski D, Aronson BD, Kading M, Morisky D. Relationship between self-efficacy and patient knowledge on adherence to oral contraceptives using the Morisky Medication Adherence Scale (MMAS-8). Reproductive Health. 2017; 14(1):110. [DOI:10.1186/s12978-017-0374-6] [PMID] [PMCID]
19.Lee TY, Cheung CK, Kwong WM. Resilience as a positive youth development construct: A conceptual review. The Scientific World Journal. 2012; 2012:390450. [DOI:10.1100/2012/390450] [PMID] [PMCID]
20.Jarab AS, Alqudah SG, Mukattash TL, Shattat G, Al-Qirim T. Randomized controlled trial of clinical pharmacy management of patients with type 2 diabetes in an outpatient diabetes clinic in Jordan. Journal of Managed Care Pharmacy. 2012; 18(7):516-26. [DOI:10.18553/jmcp.2012.18.7.516] [PMID]
21.Karthickeyan K, Panneerselvam P, Thomas A, Kameswaran R, Krishnaveni K, Srinivasan S. Assessment of Therapeutic Outcome and Medication Adherence in Diabetics Consumed Insulin, Oral Hypoglycemics and poly herbal drugs. Journal of Young Pharmacists. 2018;10(2):226-30. [DOI:10.5530/jyp.2018.10.50]
22.Lauffenburger JC, Lewey J, Jan S, Makanji S, Ferro CA, Krumme AA, et al. Effectiveness of targeted insulin-adherence interventions for glycemic control using predictive analytics among patients with type 2 diabetes: A randomized clinical trial. JAMA network open. 2019; 2(3):e190657. [DOI:10.1001/jamanetworkopen.2019.0657] [PMID] [PMCID]
23.Cassimatis M, Kavanagh DJ. Effects of type 2 diabetes behavioural telehealth interventions on glycaemic control and adherence: A systematic review. Journal of telemedicine and telecare. 2012; 18(8):447-50. [DOI:10.1258/jtt.2012.gth105] [PMID]
24.Pressler SJ, Kim J, Riley P, Ronis DL, Gradus-Pizlo I. Memory dysfunction, psychomotor slowing, and decreased executive function predict mortality in patients with heart failure and low ejection fraction. Journal of Cardiac Failure. 2010; 16(9):750-60. [DOI:10.1016/j.cardfail.2010.04.007] [PMID] [PMCID]
25.van der Wal MH, Jaarsma T, van Veldhuisen DJ. Non-compliance in patients with heart failure; how can we manage it? European Journal of Heart Failure. 2005; 7(1):5-17. [DOI:10.1016/j.ejheart.2004.04.007] [PMID]
Received: 2019/03/17 | Accepted: 2019/09/10 | Published: 2019/11/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Hamadan University of Medical Sciences.
Published by UMSHA Press
Journal Tel: +989025126654
Publisher Tel: +985138419434
Website: http://ajnpp.umsha.ac.ir
Email: avicennajnpp[at]gmail.com
