

Volume 5, Issue 4 (November 2018)
Avicenna J Neuro Psycho Physiology 2018, 5(4): 169-178 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Esmaeilnia M, Dousti Y, Mirzaian B. The Role of Early Maladaptive Schema and Perfectionism on Body Dysmorphic Disorder Mediating Through Thought Fusion, Meta-worry, Anxiety, and Attributional Style: A Structural Model. Avicenna J Neuro Psycho Physiology 2018; 5 (4) :169-178
URL: http://ajnpp.umsha.ac.ir/article-1-139-en.html
URL: http://ajnpp.umsha.ac.ir/article-1-139-en.html


1- Department of Psychology, Faculty of Humanities, Sari Branch Islamic Azad University, Sari, Iran.
2- Department of Psychology, Faculty of Humanities, Sari Branch Islamic Azad University, Sari, Iran. , dousti@iausari.ac.ir
2- Department of Psychology, Faculty of Humanities, Sari Branch Islamic Azad University, Sari, Iran. , dousti@iausari.ac.ir
Full-Text [PDF 811 kb]
(989 Downloads)
| Abstract (HTML) (2625 Views)

Full-Text: (1054 Views)
1. Introduction
Appearance is an essential part of a person’s identity in social situations and is immediately manifested; therefore, the significance of this structure is obvious. Also, the emphasis of the community and the public media on the apparent attractiveness makes people more sensitive to this issue. On the other hand, a negative evaluation by others leads to a feeling of dissatisfaction with one’s appearance and aggravation of this state can lead to clinical disturbances [1]. According to studies, almost all people do not like some aspects of their appearances and try to be different. The estimated prevalence of body dysmorphic disorder varies widely from 1.9% to 11.2% in various reports [2].
Different research findings indicate that the worry of the dysmorphic body is predictive of a tendency to plastic surgery [3]. Body Dysmorphic Disorder (BDD) is a psychological condition defined by three characteristics of obsessive-compulsive disorder, stress, and functional impairment [4]. The first step to reduce or treat a problem is to identify its underlying factors. In this regard, the present study seeks to provide a model to explain the direct and indirect role of early maladaptive schemes and perfectionism on BDD mediating through thought fusion, meta-worry, anxiety, and attributional style.
Academic theories show that cognitive impairments, avoidance and immune behaviors lead to the emergence and continuation of symptoms of psychiatric disorders. Hence, one of the main factors influencing BDD is the early maladaptive schema [5]. Individuals form schemas about the social world through childhood interpersonal relationships. These schemas affect the interpretation of the subsequent experiences and play a major role in thinking, feeling, behaving, and communicating with others, and inevitably and in contradict way brings adult life into the unpleasant of childhood, often have been harmful to people [6].
Thus, schemas and the early relationships of the individuals influence the development of their personality and later on act as a filter in the interpretation of social signs. In various social situations, the incompatible schema is activated and, through a defective cycle, leads to a persistent BDD [7]. In this regard, several studies have shown a relationship between BDD and maladaptive schemas [8].
Perfectionism is a personality trait and plays a vital role in the pathology and continuity of psychopathology [9]. Choo and Cha research [10] has shown that perfectionism can predict the satisfaction of individuals from their body image. Many studies show the relationship between meta-cognitive components and BDD [11, 12]. Explanatory attributional style theory provides a framework for examining optimism and pessimism constructs and suggests that some structures utilize the concept of learning disability. Attribution theorists tend to interpret the world around them in such a way to have more control over it [13]. In general, reviews have shown that attributional interpretations play a decisive role in accepting responsibility for their actions or forcing others to take responsibility [14]. Fisak et al. showed that people with dysmorphic disorders avoid social situations and friendships [15].
Anxiety is another variable that can play a role in the onset and severity of BDD. Several studies have shown the association between physical dissatisfaction with anxiety and stress and obsessive-compulsive behaviors [16]. People with BDD are anxious and worried about their perceived defects in various areas of life. The onset of intrusive or unwanted images and thoughts on physical appearance has diminished the quality of life and the daily functioning of these people [17]. In Martens et al. study [18], the perception of BDD has been associated with depression and anxiety. Thus, there is a positive correlation between early maladaptive schemas, perfectionism, thought blending, meta-worry, anxiety, and attributional style. However, these relationships are not explicitly mentioned in previous studies. Also, the indirect role of the psychological factors studied in this research has been studied even less.
Based on these findings, the direct and indirect association of the early maladaptive schemas and perfectionism with thought fusion, meta-worry, anxiety, and attributional style are not evident. Therefore, this research aimed to investigate these relationships. In other words, can we consider a mediating role for the thought fusion, meta-worry, anxiety, and attributional style on the symptoms of BDD? Or does the conceptual model fit with the measured model?
2. Materials and Methods
The present research regarding the topic, goals, and hypotheses is a descriptive correlational study, which was implemented using a structural equation model. The statistical population included all women referring to Ghaemshahr Dermatology centers in the spring and summer of 2018. A sample of 300 patients was selected from these women based on purposeful sampling and the number of study variables. For each variable, 50 individuals were sampled and selected. After selecting the samples, the questionnaires were administered to them. Also, they were told that it is not necessary to mention their names in the questionnaires. The participants signed their written consent before they started, and the results would be interpreted if desired. In this way, oral and written consent was obtained.
For data collection, we used the BDD questionnaire, a short version of the early maladaptive schema, perfectionism, anxiety test, thought event fusion, attributional style questionnaire, and anxious thought inventory questionnaire. After collecting questionnaires and extracting data, descriptive indicators of dispersion and central tendency, especially mean and the standard deviation were used to sort out the raw data. Next, structural equation modeling was used to analyze the obtained data related to the research hypothesis. Accordingly, first, the correlation coefficient of the studied variables was calculated and then, the measured model in the form of structural relationships between variables was investigated by structural equation modeling. To collect the study data, we used seven research tools Table 1.
Body Dysmorphic Disorder Questionnaire
Phillips et al. developed this questionnaire in 1997, and it has 31 questions. It aimed to evaluate the meta-cognitive dimensions of the dysmorphic body, meta-cognitive control strategies, thought-action coalitions, or thought event fusion, positive and negative metacognitive beliefs, and safety behaviors. The questionnaire is rated based on a 5-point Likert-type scale (from 1-5). In Rabi’i et al. study of concurrent validity on 200 students showed that the dysmorphic body meta-cognition assessment questionnaire and its factors have a positive and significant correlation with the corrected Yale-Brown obsessive-compulsive scales for BDD [15]. The validity and reliability of this questionnaire in this study were 0.72 and 0.70, respectively [15].
Young Schema Questionnaire Short Form
Young and Brown designed this questionnaire in 1998, and the original form has 205 items [19]. Later on, a short form of the questionnaire was developed. Each item is graded on a 6-point scale. In this questionnaire, every 5 questions will measure a schema. In Colburn et al. study, all 15 subscales of the short form of the schema questionnaire had a sufficiently good internal consistency. The Cronbach alpha values of all schemas were calculated from 0.76 to 0.93. Also, the reliability of the short form of the questionnaire was reciprocated using a reciprocal method of 0.44 [20]. The validity and reliability of this questionnaire were 0.74 and 0.77, respectively.
Thought Event Fusion Test
This is a self-assessment test with 14 items that measures common beliefs about the meaning and power of thoughts. This test assesses the three categories of thought-event fusion that are introduced in the meta-cognitive model. These three factors are the thought-action fusion, the thought object fusion, and the thought event fusion. Answers are rated based on a 100-point continuum (from 0 “I do not believe” to 100 “I totally believe”) and ranked as ten. Few studies have reported the psychometric properties of the thought event fusion test, including William who reported an adequate internal consistency coefficient for this questionnaire (Cronbach's alpha = 0.89). The total correlation between the items ranges from 0.35 to 0.78 [21]. Also, research studies have shown correlations of 0.4 to 0.7 between this test and metacognitive beliefs and thought-action fusion questionnaire [19]. To calculate convergent validity, a revised questionnaire of thought-action fusion was used which in terms of the cognitive concept is most similar to this test. The correlation coefficient between the two questionnaires was 0.65 [22].
Positive and Negative Perfectionism Scale
This 40-item scale was developed by Terry-Short et al. [23]. Twenty items measure positive perfectionism, and 20 other items the negative perfectionism. Questions are rated based on a 5-point Likert-type scale from score 1 to score 5 in two positive and negative fields. The minimum score for each of the test scales is 20 and the maximum is 100. In the Persian version of this questionnaire, the Cronbach alpha of the questions of each subscale in a sample of 212 students were 90% and 87% for all subjects; 91% and 88% for female students, 89% and 86% for male students, indicating the high internal consistency of the scale [24].
Spielberger Anxiety Test
Spielberger introduced the first form of the adjectival and state-of-the-art test in 1970 and revised it in 1983 [25]. The reliability level for the norm group (600 people) based on the Cronbach alpha in the open and hidden anxiety scale are 0.90 and 0.91, respectively, and 0.94 in the criterion group (130). Besides, the reliability of the test was calculated through the ratio of the variance of the actual scores to the observed variance, and its value was recorded in the normal group as 0.945 [26]. The validity and reliability of this questionnaire in this study were found as 0.75 and 0.73, respectively.
Anxiety Thinking Questionnaire (Meta-worry)
Wells introduced this questionnaire in 1994 [27]. The questionnaire consists of 22 items and measures anxiety thoughts. The components of this questionnaire are health concerns, social concerns, and meta-worry. The validity of the questionnaire has been examined by its correlation method. Regarding the reliability, the Cronbach alpha coefficient of the whole questionnaire was 91% [28].
Attributional Style Questionnaire
Peterson and Seligman (1984) developed this questionnaire to measure personal attributes for uncontrollable events. Attributional style questionnaire consists of twelve hypothetical positions (six good events and six bad events). Four questions have been raised for each event. The first question is about the most important cause of this event, although not used in grading, is necessary for the subject to respond to the following three questions on the internal or external, stable or unstable, and general or specific events. Bridges (2001) reported the Cronbach alpha coefficient of 0.8 for the attributional style questionnaire [29].
3. Results
The obtained data are presented by the central tendency and dispersion, the mean and standard deviation. The Kolmogorov-Smirnov test was applied to check the normal distribution of the study variables.
Appearance is an essential part of a person’s identity in social situations and is immediately manifested; therefore, the significance of this structure is obvious. Also, the emphasis of the community and the public media on the apparent attractiveness makes people more sensitive to this issue. On the other hand, a negative evaluation by others leads to a feeling of dissatisfaction with one’s appearance and aggravation of this state can lead to clinical disturbances [1]. According to studies, almost all people do not like some aspects of their appearances and try to be different. The estimated prevalence of body dysmorphic disorder varies widely from 1.9% to 11.2% in various reports [2].
Different research findings indicate that the worry of the dysmorphic body is predictive of a tendency to plastic surgery [3]. Body Dysmorphic Disorder (BDD) is a psychological condition defined by three characteristics of obsessive-compulsive disorder, stress, and functional impairment [4]. The first step to reduce or treat a problem is to identify its underlying factors. In this regard, the present study seeks to provide a model to explain the direct and indirect role of early maladaptive schemes and perfectionism on BDD mediating through thought fusion, meta-worry, anxiety, and attributional style.
Academic theories show that cognitive impairments, avoidance and immune behaviors lead to the emergence and continuation of symptoms of psychiatric disorders. Hence, one of the main factors influencing BDD is the early maladaptive schema [5]. Individuals form schemas about the social world through childhood interpersonal relationships. These schemas affect the interpretation of the subsequent experiences and play a major role in thinking, feeling, behaving, and communicating with others, and inevitably and in contradict way brings adult life into the unpleasant of childhood, often have been harmful to people [6].
Thus, schemas and the early relationships of the individuals influence the development of their personality and later on act as a filter in the interpretation of social signs. In various social situations, the incompatible schema is activated and, through a defective cycle, leads to a persistent BDD [7]. In this regard, several studies have shown a relationship between BDD and maladaptive schemas [8].
Perfectionism is a personality trait and plays a vital role in the pathology and continuity of psychopathology [9]. Choo and Cha research [10] has shown that perfectionism can predict the satisfaction of individuals from their body image. Many studies show the relationship between meta-cognitive components and BDD [11, 12]. Explanatory attributional style theory provides a framework for examining optimism and pessimism constructs and suggests that some structures utilize the concept of learning disability. Attribution theorists tend to interpret the world around them in such a way to have more control over it [13]. In general, reviews have shown that attributional interpretations play a decisive role in accepting responsibility for their actions or forcing others to take responsibility [14]. Fisak et al. showed that people with dysmorphic disorders avoid social situations and friendships [15].
Anxiety is another variable that can play a role in the onset and severity of BDD. Several studies have shown the association between physical dissatisfaction with anxiety and stress and obsessive-compulsive behaviors [16]. People with BDD are anxious and worried about their perceived defects in various areas of life. The onset of intrusive or unwanted images and thoughts on physical appearance has diminished the quality of life and the daily functioning of these people [17]. In Martens et al. study [18], the perception of BDD has been associated with depression and anxiety. Thus, there is a positive correlation between early maladaptive schemas, perfectionism, thought blending, meta-worry, anxiety, and attributional style. However, these relationships are not explicitly mentioned in previous studies. Also, the indirect role of the psychological factors studied in this research has been studied even less.
Based on these findings, the direct and indirect association of the early maladaptive schemas and perfectionism with thought fusion, meta-worry, anxiety, and attributional style are not evident. Therefore, this research aimed to investigate these relationships. In other words, can we consider a mediating role for the thought fusion, meta-worry, anxiety, and attributional style on the symptoms of BDD? Or does the conceptual model fit with the measured model?
2. Materials and Methods
The present research regarding the topic, goals, and hypotheses is a descriptive correlational study, which was implemented using a structural equation model. The statistical population included all women referring to Ghaemshahr Dermatology centers in the spring and summer of 2018. A sample of 300 patients was selected from these women based on purposeful sampling and the number of study variables. For each variable, 50 individuals were sampled and selected. After selecting the samples, the questionnaires were administered to them. Also, they were told that it is not necessary to mention their names in the questionnaires. The participants signed their written consent before they started, and the results would be interpreted if desired. In this way, oral and written consent was obtained.
For data collection, we used the BDD questionnaire, a short version of the early maladaptive schema, perfectionism, anxiety test, thought event fusion, attributional style questionnaire, and anxious thought inventory questionnaire. After collecting questionnaires and extracting data, descriptive indicators of dispersion and central tendency, especially mean and the standard deviation were used to sort out the raw data. Next, structural equation modeling was used to analyze the obtained data related to the research hypothesis. Accordingly, first, the correlation coefficient of the studied variables was calculated and then, the measured model in the form of structural relationships between variables was investigated by structural equation modeling. To collect the study data, we used seven research tools Table 1.
Body Dysmorphic Disorder Questionnaire
Phillips et al. developed this questionnaire in 1997, and it has 31 questions. It aimed to evaluate the meta-cognitive dimensions of the dysmorphic body, meta-cognitive control strategies, thought-action coalitions, or thought event fusion, positive and negative metacognitive beliefs, and safety behaviors. The questionnaire is rated based on a 5-point Likert-type scale (from 1-5). In Rabi’i et al. study of concurrent validity on 200 students showed that the dysmorphic body meta-cognition assessment questionnaire and its factors have a positive and significant correlation with the corrected Yale-Brown obsessive-compulsive scales for BDD [15]. The validity and reliability of this questionnaire in this study were 0.72 and 0.70, respectively [15].
Young Schema Questionnaire Short Form
Young and Brown designed this questionnaire in 1998, and the original form has 205 items [19]. Later on, a short form of the questionnaire was developed. Each item is graded on a 6-point scale. In this questionnaire, every 5 questions will measure a schema. In Colburn et al. study, all 15 subscales of the short form of the schema questionnaire had a sufficiently good internal consistency. The Cronbach alpha values of all schemas were calculated from 0.76 to 0.93. Also, the reliability of the short form of the questionnaire was reciprocated using a reciprocal method of 0.44 [20]. The validity and reliability of this questionnaire were 0.74 and 0.77, respectively.
Thought Event Fusion Test
This is a self-assessment test with 14 items that measures common beliefs about the meaning and power of thoughts. This test assesses the three categories of thought-event fusion that are introduced in the meta-cognitive model. These three factors are the thought-action fusion, the thought object fusion, and the thought event fusion. Answers are rated based on a 100-point continuum (from 0 “I do not believe” to 100 “I totally believe”) and ranked as ten. Few studies have reported the psychometric properties of the thought event fusion test, including William who reported an adequate internal consistency coefficient for this questionnaire (Cronbach's alpha = 0.89). The total correlation between the items ranges from 0.35 to 0.78 [21]. Also, research studies have shown correlations of 0.4 to 0.7 between this test and metacognitive beliefs and thought-action fusion questionnaire [19]. To calculate convergent validity, a revised questionnaire of thought-action fusion was used which in terms of the cognitive concept is most similar to this test. The correlation coefficient between the two questionnaires was 0.65 [22].
Positive and Negative Perfectionism Scale
This 40-item scale was developed by Terry-Short et al. [23]. Twenty items measure positive perfectionism, and 20 other items the negative perfectionism. Questions are rated based on a 5-point Likert-type scale from score 1 to score 5 in two positive and negative fields. The minimum score for each of the test scales is 20 and the maximum is 100. In the Persian version of this questionnaire, the Cronbach alpha of the questions of each subscale in a sample of 212 students were 90% and 87% for all subjects; 91% and 88% for female students, 89% and 86% for male students, indicating the high internal consistency of the scale [24].
Spielberger Anxiety Test
Spielberger introduced the first form of the adjectival and state-of-the-art test in 1970 and revised it in 1983 [25]. The reliability level for the norm group (600 people) based on the Cronbach alpha in the open and hidden anxiety scale are 0.90 and 0.91, respectively, and 0.94 in the criterion group (130). Besides, the reliability of the test was calculated through the ratio of the variance of the actual scores to the observed variance, and its value was recorded in the normal group as 0.945 [26]. The validity and reliability of this questionnaire in this study were found as 0.75 and 0.73, respectively.
Anxiety Thinking Questionnaire (Meta-worry)
Wells introduced this questionnaire in 1994 [27]. The questionnaire consists of 22 items and measures anxiety thoughts. The components of this questionnaire are health concerns, social concerns, and meta-worry. The validity of the questionnaire has been examined by its correlation method. Regarding the reliability, the Cronbach alpha coefficient of the whole questionnaire was 91% [28].
Attributional Style Questionnaire
Peterson and Seligman (1984) developed this questionnaire to measure personal attributes for uncontrollable events. Attributional style questionnaire consists of twelve hypothetical positions (six good events and six bad events). Four questions have been raised for each event. The first question is about the most important cause of this event, although not used in grading, is necessary for the subject to respond to the following three questions on the internal or external, stable or unstable, and general or specific events. Bridges (2001) reported the Cronbach alpha coefficient of 0.8 for the attributional style questionnaire [29].
3. Results
The obtained data are presented by the central tendency and dispersion, the mean and standard deviation. The Kolmogorov-Smirnov test was applied to check the normal distribution of the study variables.
Table 2 presents the path coefficients and the significant effects of the direct impact. The results indicate that in the direct model (the study of the direct relation between predictive variables with criterion variables), the causal paths toward the dysmorphic body, early maladaptive schemes, perfectionism, thought fusion, attributional style, anxiety, and meta-worry have positive and significant roles. It is worth mentioning that among these factors, the load factor of thought fusion and meta-worry is more than other factors.
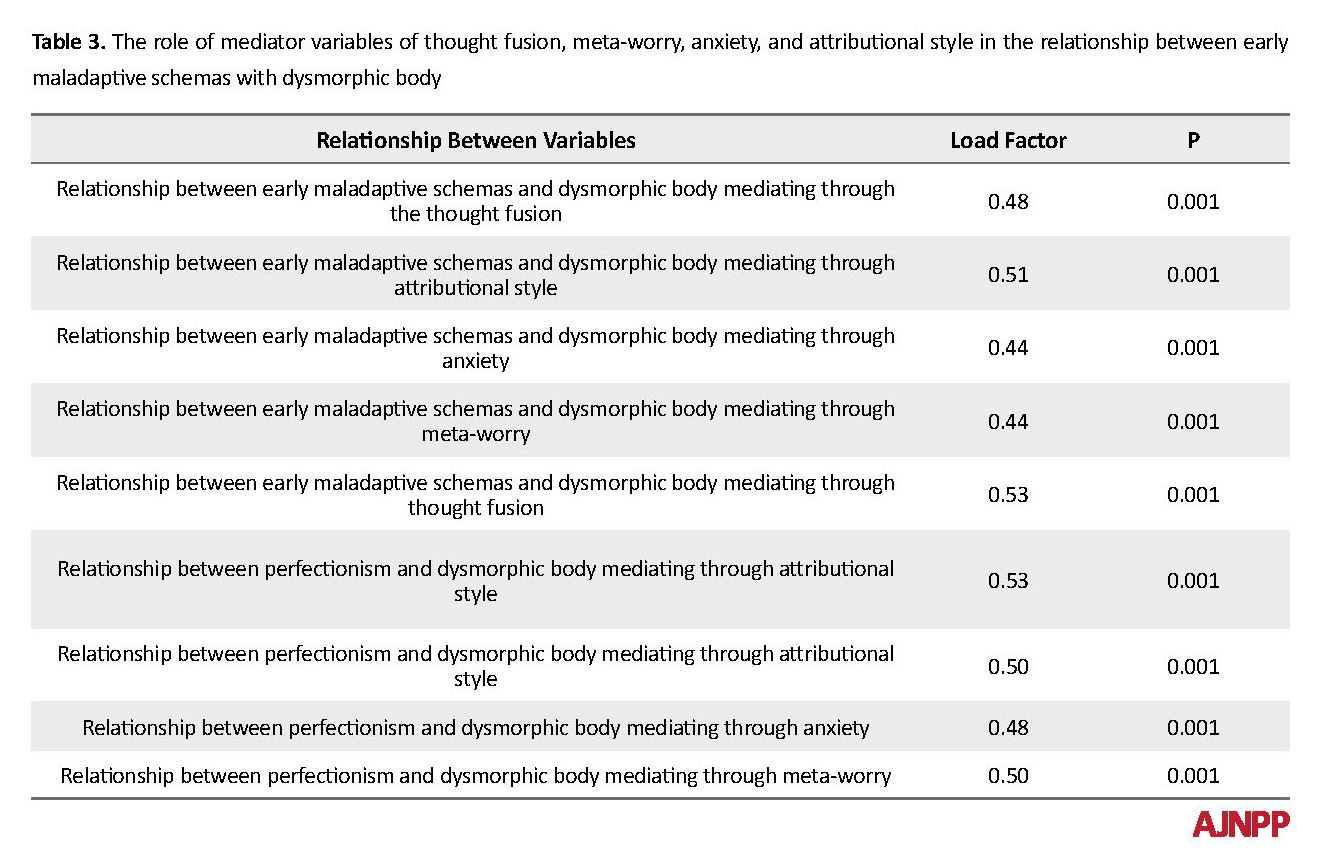
Table 3 presents the path coefficients and significant indirect effects. The results point out that in the indirect model (investigating the indirect relationship between predictor and criterion variables with intermediary variables), the causal paths toward the components of thought fusion, attributional style, anxiety, and meta-worry with perfectionism and early maladaptive schema have a positive and significant relationship. In causal paths toward the dysmorphic body, the thought fusion relation, attributional style, anxiety, and meta-worry are positively and significantly related to BDD.
The measured model is fitted with the theoretical model because the standard error estimate is less than 0.05. On the other hand, the value of goodness fit index, the goodness of modified fitness, goodness adjusted fitness index, softened index of fitness, softness index, and fitness of good index of increasing fit are all higher than optimal (0.90). Therefore, the structural relationships of the early maladaptive schemes and perfectionism with the BDD are significant with the mediation of thought fusion, attributional style, anxiety, and meta-worry. In other words, thought fusion, attributional style, anxiety, and meta-worry can mediate the relationships between early maladaptive schemas and perfectionism with BDD.
4. Discussion
In this study, the direct and indirect effects of two variables of early maladaptive schema and perfectionism with mediating of thought fusion, attributional style, anxiety, and meta-worry on BDD were studied. The results of the research showed an appropriate fit between the data and the model. In general, this study aimed to examine the cognitive, meta-cognitive, and emotional processes involved in body dysmorphic disorder. The results of the research hypotheses include the following findings.
There is a direct correlation between the BDD and the early maladaptive schemas. This finding is consistent with other research findings [8]. In explaining this finding, it can be stated that the early maladaptive schema is associated with psychological stresses, experiences, and negative life events, and these schemas, directly and indirectly, lead to the formation and chronicization of various forms of mental disturbances.
Perfectionism directly affects BDD. This finding is consistent with other research findings [10]. In explaining the results of this hypothesis, it can be assumed that people with BDD tend to think and behave in a more perfectionist way than others. So based on this assumption, they even pay attention to the minor defects and focus on them. And, when they are unable to withstand their defects, this leads to bad feelings and turmoil [30].
Thought fusion directly affects the BDD. This finding is consistent with other research findings [11]. In explaining the findings of this hypothesis, Wells and Matthews metacognitive theory can be mentioned [32], which is a combination of schema theory and information processing theory and emphasizes one’s beliefs about the processing system. Based on metacognitive patterns, obsessive thoughts are due to metacognitive beliefs about the meaning or the dangerous consequences of having such thoughts that are negatively interpreted and explained.
Meta-worry directly affects BDD. This finding is consistent with the results of other research studies [11]. Anxiety directly affects BDD, too. This finding is consistent with other research results [33]. In explaining the findings of this hypothesis, it can be argued that patients with BDD experience anxiety about how they appear. Continuous mental engagement of patients about physical appearance can cause a lot of anxiety. Given that patients experience severe anxiety about their physical appearances, they rely on avoidance and safety behaviors to control anxiety and stress. These behaviors may temporarily reduce anxiety and, on the other hand, enhance the person’s self-esteem as well as frequent use of avoidance and safety behaviors.
The attributional style directly affects body dysmorphic disorder. This finding is consistent with other research findings from the research of Dykas and Cassidy [34]. According to the results of this hypothesis, people with BDD, in social situations and interactions, show a more cynical interpretation and negative experiences related to appearance. They interpret their physical senses more often based on the negative attributional style. Indeed, their negative experiences give rise to internal, sustained, and general factors.
The early maladaptive schema indirectly affects BDD mediating through thought fusion. This finding is consistent with other research findings [35]. In explaining the results of the present study, we can point out the findings of Cormier et al. [36] that when initial maladaptive schemas are activated, they can affect perception, reality and cognitive processing of the individual.
The early maladaptive schema also indirectly affects the BDD by mediating through meta-worry. In the literature, there is no direct research in this regard. In the explanation of this hypothesis, we can say that meta-worry occurs when a person is afraid of his or her negative cognitive knowledge and considers them unnatural and only specify them to his or her mind [37]. When people are so scared of their thoughts and find them as abnormal and uncontrollable, they become more afraid of themselves. At the same time, they ignore or control their thoughts because of fear and stress [31]. Therefore, in this context, worry as a processing strategy may lead to the spread of disturbing thoughts.
The features of the early maladaptive schema affect BDD indirectly by mediating anxiety. This finding is consistent with other research findings [38]. In explaining the results of this hypothesis, it seems to be compatible with the increasing social relationships of individuals, especially women, in the current society. Moreover, given that the early maladaptive schemas are the primary cornerstone of various types of mental disorders, including anxiety problems, as an activator of human behavior and as a response to different situations, it can lead to the anxiety of the individuals.
The features of the early maladaptive schema have an indirect impact on BDD by mediating through attributional style. In the literature, there is no direct research in this regard. In explaining the results of this hypothesis, it can be stated that early maladaptive schema with negative evaluation experience in social situations, and the resulting negative attributions may cause misjudge of the others’ behaviors about his or her appearance, and will lead to negative emotional-cognitive experiences.
Perfectionism has an indirect impact on BDD by mediating through thought fusion. This finding is consistent with other research findings [39]. It can be concluded that the relationship between perfectionism and dysmorphic body is not a simple linear relationship, and meta-cognitive beliefs such as the thought fusion can affect this relationship. Given the fact that the problems of metacognitive beliefs and perfectionism are common features of most psychological disorders, they can also be considered in explaining the BDD.
Perfectionism features indirectly affect BDD through meta-worry mediation. This finding is consistent with the results of other studies [39]. The explanation of the results of this hypothesis can be found in the research findings of Molding and Kyrios [40]. They argued that beliefs such as the sense of extreme responsibility, the high concern about the importance of controlling thoughts, certainty, and idealism (perfectionism) are merely related to a person’s extreme intention to managing events and outcomes. Moreover, this leads to an exaggeration of threat assessment and is often linked to individual cognitive control over results.
Perfectionism features indirectly affect BDD by mediating through anxiety. This finding is consistent with other research results [41]. Based on the findings of this hypothesis, we conclude that perfectionism makes a person experience extreme negative emotions, especially anxiety. This arousal causes the patient to experience more disturbing thoughts and feelings about the symptoms of body deformity. Because of creating pressure and tension, this stimulus prevents a realistic assessment of disturbing thoughts and feelings, and unpleasant emotions and negative emotions continue. In other words, these metacognitive beliefs lead to the formation of ineffective behaviors that may last for hours. Thus, to deal with perceived risk, the practice of safety behaviors (such as medical and various surgical procedures) is aggravated.
Perfectionism features have indirect effects on BDD by mediating through the attributional style. This finding is consistent with the results of other research studies [42]. For perfectionists, the result is so important that they press upon themselves exceptionally hard to reach their goals. It seems that perfectionists who have a negative attributional style interpreted unpleasant events more negatively, and on the other hand, with their stubborn criteria and the inflexibility of their underlying beliefs, they have a significant effect on the aggravation of problems related to physical appearance dissatisfaction.
5. Conclusion
The early maladaptive schema and perfectionism have a predictive role in BDD mediating through thought fusion, meta-worry, anxiety, and attributional style.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the research objectives and its procedure and signed the informed consent. They were also assured about the confidentiality of their information, and allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interests.
References
Phillips KA. Body dysmorphic disorder: common, severe and in need of treatment research. Psychotherapy and psychosomatics. 2014; 83(6):325-9. [DOI:10.1159/000366035] [PMID]
Veale D, Gledhill LJ, Christodoulou P, Hodsoll J. Body dysmorphic disorder in different settings: A systematic review and estimated weighted prevalence. Body Image. 2016; 18:168-86. [DOI:10.1016/j.bodyim.2016.07.003] [PMID]
Dey JK, Ishii M, Phillis M, Byrne PJ, Boahene KD, Ishii LE. et al. Body dysmorphic disorder in a facial plastic and reconstructive surgery clinic: Measuring prevalence, assessing comorbidities, and validating a feasible screening instrument. JAMA Facial Plastic Surgery. 2015; 17(2):137-43. [DOI:10.1001/jamafacial.2014.1492] [PMID]
Hartmann AS, Thomas JJ, Wilson AC, Wilhelm S. Insight impairment in body image disorders: Delusionality and overvalued ideas in anorexia nervosa versus body dysmorphic disorder. Psychiatry Research. 2013; 210(3):1129-35. [DOI:10.1016/j.psychres.2013.08.010] [PMID]
Farmer AS, Kashdan TB. Social anxiety and emotion regulation in daily life: Spillover effects on positive and negative social events. Cognitive Behaviour Therapy. 2012; 41(2):152-62. [DOI:10.1080/16506073.2012.666561] [PMID] [PMCID]
Masley SA, Gillanders DT, Simpson SG, Taylor MA. A systematic review of the evidence base for schema therapy. Cognitive Behaviour Therapy. 2012; 41(3):185-202. [DOI:10.1080/16506073.2011.614274] [PMID]
Hinrichsen H, Waller G, Emanuelli F. Social anxiety and agoraphobia in the eating disorders: associations with core beliefs. The Journal of Nervous and Mental Disease. 2004; 192(11):784-7. [DOI:10.1016/j.eatbeh.2004.04.008] [PMID]
Boone L, Braet C, Vandereycken W. Are maladaptive schema domains and perfectionism related to body image concerns in eating disorder patients. European Eating Disorders Review. 2013: 21(1):45-51. [DOI:10.1002/erv.2175] [PMID]
Shafran R, Mansel W. Perfectionism psychopathology: A review of research and treatment. Clinical Psychology Review. 2001; 21:819-906. [DOI:10.1016/S0272-7358(00)00072-6]
Choo SY, Cha CKY. Predicting eating problems among Malaysian Chinese: Differential roles of positive and negative perfectionism. Personality and individual differences. 2013; 54(6):744-9. [DOI:10.1016/j.paid.2012.11.036]
Rabiei M, Mulkens S, Kalantari M, Molavi H, Bahrami F. Metacognitive therapy for body dysmorphic disorder patients in Iran: acceptability and proof of concept. Journal of behavior therapy and experimental psychiatry. 2012; 43(2):724-9. [DOI:10.1016/j.jbtep.2011.09.013] [PMID]
Veale D, Anson M, Miles S, Pieta M, Costa A, Ellison N. Efficacy of cognitive behaviour therapy versus anxiety management for body dysmorphic disorder: a randomised controlled trial. Psychotherapy and psychosomatics. 2014; 83(6):341-53. [DOI:10.1159/000360740] [PMID]
Zeinodini Z, Sedighi S, Rahimi MB, Noorbakhsh S, Esfahani SR. Dysfunctional metacognitive beliefs in body dysmorphic disorder. Global journal of health science. 2016; 8(3):10. [DOI:10.5539/gjhs.v8n3p10] [PMID] [PMCID]
Harrison A, de la Cruz LF, Enander J, Radua J, Mataix-Cols D. Cognitive-behavioral therapy for body dysmorphic disorder: A systematic review and meta-analysis of randomized controlled trials. Clinical Psychology Review. 2016; 48:43-51. [DOI:10.1016/j.cpr.2016.05.007] [PMID]
Fisak B, Mentuccia M, Przeworski A. Meta-worry in adolescents: Examination of the psychometric properties of the meta-worry questionnaire in an adolescent sample. Behavioural and cognitive psychotherapy. 2014; 42(4):491-6. [DOI:10.1017/S1352465813000374] [PMID]
Benedict C, Rodriguez VM, Carter J, Temple L, Nelson C, Duhamel K. Investigation of body image as a mediator of the effects of bowel and GI symptoms on psychological distress in female survivors of rectal and anal cancer. Support Care Cancer. 2016; 24(4):1795-802. [DOI:10.1007/s00520-015-2976-2] [PMID] [PMCID]
Hofmann SG, Asnaani A, Vonk IJ, Sawyer AT, Fang A. The efficacy of cognitive behavioral therapy: A review of meta-analyses. Cognitive therapy and research. 2012; 36(5):427-40. [DOI:10.1007/s10608-012-9476-1] [PMID] [PMCID]
Martens U, Czerwenka S, Schrauth M, Kowalski A, Enck P, Hartmann M, et al. Body image and psychiatric comorbidity in patients with somatoform gastrointestinal disorders. Zeitschrift fur Psychosomatische Medizin und Psychotherapie. 2010; 56(1):47-55. [DOI:10.13109/zptm.2010.56.1.47] [PMID]
Kriston L, Schäfer J, Jacob GA, Härter M, Hölzel LP. Reliability and validity of the German version of the Young Schema Questionnaire-Short Form 3 (YSQ-S3). European Journal of Psychological Assessment. 2013; 29:205-12. [DOI:10.1027/1015-5759/a000143]
Welburn K, Coristine M, Dagg P, Pontefract A, Jordan SH. The schema questionnaire - short form: factor analysis and the relationship between schemas and symptoms. Cognitive Therapy and Research. 2002: 26(4):519-30. [DOI:10.1023/A:1016231902020]
Williams J, Hadjistavropoulos T, Sharpe D. A meta-analysis of psychological and pharmacological treatments for body dysmorphic disorder. Behaviour Research and Therapy. 2006; 44(1):99-111. [DOI:10.1016/j.brat.2004.12.006] [PMID]
Shafrana R, Rachman S. Thought-action fusion: a review. Journal of Behavior Therapy and Experimental Psychiatry. 2004; 35(4):87-107. [DOI:10.1016/j.jbtep.2004.04.002] [PMID]
Kung CS, Chan CK. Differential roles of positive and negative perfectionism in predicting occupational eustress and distress. Personality and Individual differences. 2014; 58:76-81. [DOI:10.1016/j.paid.2013.10.011]
Short MM, Mazmanian D. Perfectionism and negative repetitive thoughts: Examining a multiple mediator model in relation to mindfulness. Personality and Individual Differences. 2013; 55(6):716-21. [DOI:10.1016/j.paid.2013.05.026]
Spielberger CD, Gonzalez-Reigosa F, Martinez-Urrutia A, Natalicio LF, Natalicio DS. The state-trait anxiety inventory. Revista Interamericana de Psicologia/Interamerican. Journal of Psychology. 2010; 17(5):3-4. [DOI:10.1002/9780470479216.corpsy0943]
Sadati L, Pazouki A, Mehdizadeh A, Shoar S, Tamannaie Z, Chaichian S. Effect of preoperative nursing visit on preoperative anxiety and postoperative complications in candidates for laparoscopic cholecystectomy: A randomized clinical trial. Scandinavian journal of caring sciences. 2013; 27(4):994-8. [DOI:10.1111/scs.12022] [PMID]
Whiting SE, May AC, Rudy BM, Davis TE. Strategies for the control of unwanted thoughts in adolescents: The Adolescent Thought Control Questionnaire (TCQ-A). Journal of Psychopathology and Behavioral Assessment. 2014; 36(2):276-87. [DOI:10.1007/s10862-013-9369-y]
Gillanders DT, Bolderston H, Bond FW, Dempster M, Flaxman PE, Campbell L, et al. The development and initial validation of the cognitive fusion questionnaire. Behavior therapy. 2014; 45(1):83-101. [DOI:10.1016/j.beth.2013.09.001] [PMID]
Bridges KR. Using attributional style to predict academic performance: How does it compare to traditional methods. Personality and individual differences. 2001; 31:723-30. [DOI:10.1016/S0191-8869(00)00174-4]
Fingeret MC, Teo I, Epner DE. Managing body image difficulties of adult cancer patients: lessons from available research. Cancer. 2014; 120(5):633-41. [DOI:10.1002/cncr.28469] [PMID] [PMCID]
Normann N, van Emmerik AA, Morina N. The efficacy of metacognitive therapy for anxiety and depression: A meta‐analytic review. Depression and Anxiety. 2014; 31(5):402-11. [DOI:10.1002/da.22273] [PMID]
Elliott R, Zahn R, Deakin JW, Anderson IM. Affective cognition and its disruption in mood disorders. Neuropsychopharmacology. 2011; 36(1):153. [DOI:10.1038/npp.2010.77] [PMID] [PMCID]
Collins B, Gonzalez D, Gaudilliere DK, Shrestha P, Girod S. Body dysmorphic disorder and psychological distress in orthognathic surgery patients. Journal of Oral and Maxillofacial Surgery. 2014; 72(8): 1553-8. [DOI:10.1016/j.joms.2014.01.011] [PMID]
Dykas MJ, Cassidy J. Attachment and the processing of social information across the life span: Theory and evidence. Psychological bulletin. 2011; 137(1):19. [DOI:10.1037/a0021367] [PMID]
Dimaggio G, Popolo R, Salvatore G. Formulation of functioning for avoidant personality disorder in metacognitive interpersonal therapy. In: Kramer U, editor. Case Formulation for Personality Disorders. Massachusetts: Academic Press; 2019. [DOI:10.1016/B978-0-12-813521-1.00008-4]
Cormier A, Jourda B, Laros C, Walburg V, Callahan S. Influence between early maladaptive schemas and depression. L’Encéphale, 2010; 37(4):293-8. [DOI:10.1016/j.encep.2011.01.001] [PMID]
Wells A, Carter K. Further tests of a cognitive model of generalized anxiety disorder: Meta-cognitions and worry in GAD, panic disorder, social phobia, depression, and nonpatients. Behavior Therapy. 2001; 32:85-102. [DOI:10.1016/S0005-7894(01)80045-9]
Lambert KG. Rising rates of depression in today’s society: Consideration of the roles of effort-based rewards and enhanced resilience in day-to-day functioning. Neuroscience & Biobehavioral Reviews. 2006; 30(4):497-510. [DOI:10.1016/j.neubiorev.2005.09.002] [PMID]
Grøtte T, Solem S, Vogel PA, Güzey IC, Hansen B, Myers SG. Metacognition, responsibility, and perfectionism in obsessive-compulsive disorder. Cognitive Therapy and Research. 2015; 39(1):41-50. [DOI:10.1007/s10608-014-9635-7]
Moulding R, Kyrios M. Anxiety disorders and control related beliefs: The exemplar of Obsessive-Compulsive Disorder (OCD). Clinical Psychology Review. 2006; 26(5):573-83. [DOI:10.1016/j.cpr.2006.01.009] [PMID]
Saboonchi F, Lundh LG. Perfectionism, anger, somatic health, and positive effect. Personality and Individual Differences. 2003; 35:1585-99. [DOI:10.1016/S0191-8869(02)00382-3]
Limburg K, Martin S, Hagger S, Egan J. The relationship between perfectionism and psychopathology: A meta‐analysis. Journal of Clinical Psychology. 2017; 73(10):1301-26. [DOI:10.1002/jclp.22435] [PMID]
The measured model is fitted with the theoretical model because the standard error estimate is less than 0.05. On the other hand, the value of goodness fit index, the goodness of modified fitness, goodness adjusted fitness index, softened index of fitness, softness index, and fitness of good index of increasing fit are all higher than optimal (0.90). Therefore, the structural relationships of the early maladaptive schemes and perfectionism with the BDD are significant with the mediation of thought fusion, attributional style, anxiety, and meta-worry. In other words, thought fusion, attributional style, anxiety, and meta-worry can mediate the relationships between early maladaptive schemas and perfectionism with BDD.
4. Discussion
In this study, the direct and indirect effects of two variables of early maladaptive schema and perfectionism with mediating of thought fusion, attributional style, anxiety, and meta-worry on BDD were studied. The results of the research showed an appropriate fit between the data and the model. In general, this study aimed to examine the cognitive, meta-cognitive, and emotional processes involved in body dysmorphic disorder. The results of the research hypotheses include the following findings.
There is a direct correlation between the BDD and the early maladaptive schemas. This finding is consistent with other research findings [8]. In explaining this finding, it can be stated that the early maladaptive schema is associated with psychological stresses, experiences, and negative life events, and these schemas, directly and indirectly, lead to the formation and chronicization of various forms of mental disturbances.
Perfectionism directly affects BDD. This finding is consistent with other research findings [10]. In explaining the results of this hypothesis, it can be assumed that people with BDD tend to think and behave in a more perfectionist way than others. So based on this assumption, they even pay attention to the minor defects and focus on them. And, when they are unable to withstand their defects, this leads to bad feelings and turmoil [30].
Thought fusion directly affects the BDD. This finding is consistent with other research findings [11]. In explaining the findings of this hypothesis, Wells and Matthews metacognitive theory can be mentioned [32], which is a combination of schema theory and information processing theory and emphasizes one’s beliefs about the processing system. Based on metacognitive patterns, obsessive thoughts are due to metacognitive beliefs about the meaning or the dangerous consequences of having such thoughts that are negatively interpreted and explained.
Meta-worry directly affects BDD. This finding is consistent with the results of other research studies [11]. Anxiety directly affects BDD, too. This finding is consistent with other research results [33]. In explaining the findings of this hypothesis, it can be argued that patients with BDD experience anxiety about how they appear. Continuous mental engagement of patients about physical appearance can cause a lot of anxiety. Given that patients experience severe anxiety about their physical appearances, they rely on avoidance and safety behaviors to control anxiety and stress. These behaviors may temporarily reduce anxiety and, on the other hand, enhance the person’s self-esteem as well as frequent use of avoidance and safety behaviors.
The attributional style directly affects body dysmorphic disorder. This finding is consistent with other research findings from the research of Dykas and Cassidy [34]. According to the results of this hypothesis, people with BDD, in social situations and interactions, show a more cynical interpretation and negative experiences related to appearance. They interpret their physical senses more often based on the negative attributional style. Indeed, their negative experiences give rise to internal, sustained, and general factors.
The early maladaptive schema indirectly affects BDD mediating through thought fusion. This finding is consistent with other research findings [35]. In explaining the results of the present study, we can point out the findings of Cormier et al. [36] that when initial maladaptive schemas are activated, they can affect perception, reality and cognitive processing of the individual.
The early maladaptive schema also indirectly affects the BDD by mediating through meta-worry. In the literature, there is no direct research in this regard. In the explanation of this hypothesis, we can say that meta-worry occurs when a person is afraid of his or her negative cognitive knowledge and considers them unnatural and only specify them to his or her mind [37]. When people are so scared of their thoughts and find them as abnormal and uncontrollable, they become more afraid of themselves. At the same time, they ignore or control their thoughts because of fear and stress [31]. Therefore, in this context, worry as a processing strategy may lead to the spread of disturbing thoughts.
The features of the early maladaptive schema affect BDD indirectly by mediating anxiety. This finding is consistent with other research findings [38]. In explaining the results of this hypothesis, it seems to be compatible with the increasing social relationships of individuals, especially women, in the current society. Moreover, given that the early maladaptive schemas are the primary cornerstone of various types of mental disorders, including anxiety problems, as an activator of human behavior and as a response to different situations, it can lead to the anxiety of the individuals.
The features of the early maladaptive schema have an indirect impact on BDD by mediating through attributional style. In the literature, there is no direct research in this regard. In explaining the results of this hypothesis, it can be stated that early maladaptive schema with negative evaluation experience in social situations, and the resulting negative attributions may cause misjudge of the others’ behaviors about his or her appearance, and will lead to negative emotional-cognitive experiences.
Perfectionism has an indirect impact on BDD by mediating through thought fusion. This finding is consistent with other research findings [39]. It can be concluded that the relationship between perfectionism and dysmorphic body is not a simple linear relationship, and meta-cognitive beliefs such as the thought fusion can affect this relationship. Given the fact that the problems of metacognitive beliefs and perfectionism are common features of most psychological disorders, they can also be considered in explaining the BDD.
Perfectionism features indirectly affect BDD through meta-worry mediation. This finding is consistent with the results of other studies [39]. The explanation of the results of this hypothesis can be found in the research findings of Molding and Kyrios [40]. They argued that beliefs such as the sense of extreme responsibility, the high concern about the importance of controlling thoughts, certainty, and idealism (perfectionism) are merely related to a person’s extreme intention to managing events and outcomes. Moreover, this leads to an exaggeration of threat assessment and is often linked to individual cognitive control over results.
Perfectionism features indirectly affect BDD by mediating through anxiety. This finding is consistent with other research results [41]. Based on the findings of this hypothesis, we conclude that perfectionism makes a person experience extreme negative emotions, especially anxiety. This arousal causes the patient to experience more disturbing thoughts and feelings about the symptoms of body deformity. Because of creating pressure and tension, this stimulus prevents a realistic assessment of disturbing thoughts and feelings, and unpleasant emotions and negative emotions continue. In other words, these metacognitive beliefs lead to the formation of ineffective behaviors that may last for hours. Thus, to deal with perceived risk, the practice of safety behaviors (such as medical and various surgical procedures) is aggravated.
Perfectionism features have indirect effects on BDD by mediating through the attributional style. This finding is consistent with the results of other research studies [42]. For perfectionists, the result is so important that they press upon themselves exceptionally hard to reach their goals. It seems that perfectionists who have a negative attributional style interpreted unpleasant events more negatively, and on the other hand, with their stubborn criteria and the inflexibility of their underlying beliefs, they have a significant effect on the aggravation of problems related to physical appearance dissatisfaction.
5. Conclusion
The early maladaptive schema and perfectionism have a predictive role in BDD mediating through thought fusion, meta-worry, anxiety, and attributional style.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the research objectives and its procedure and signed the informed consent. They were also assured about the confidentiality of their information, and allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interests.
References
Phillips KA. Body dysmorphic disorder: common, severe and in need of treatment research. Psychotherapy and psychosomatics. 2014; 83(6):325-9. [DOI:10.1159/000366035] [PMID]
Veale D, Gledhill LJ, Christodoulou P, Hodsoll J. Body dysmorphic disorder in different settings: A systematic review and estimated weighted prevalence. Body Image. 2016; 18:168-86. [DOI:10.1016/j.bodyim.2016.07.003] [PMID]
Dey JK, Ishii M, Phillis M, Byrne PJ, Boahene KD, Ishii LE. et al. Body dysmorphic disorder in a facial plastic and reconstructive surgery clinic: Measuring prevalence, assessing comorbidities, and validating a feasible screening instrument. JAMA Facial Plastic Surgery. 2015; 17(2):137-43. [DOI:10.1001/jamafacial.2014.1492] [PMID]
Hartmann AS, Thomas JJ, Wilson AC, Wilhelm S. Insight impairment in body image disorders: Delusionality and overvalued ideas in anorexia nervosa versus body dysmorphic disorder. Psychiatry Research. 2013; 210(3):1129-35. [DOI:10.1016/j.psychres.2013.08.010] [PMID]
Farmer AS, Kashdan TB. Social anxiety and emotion regulation in daily life: Spillover effects on positive and negative social events. Cognitive Behaviour Therapy. 2012; 41(2):152-62. [DOI:10.1080/16506073.2012.666561] [PMID] [PMCID]
Masley SA, Gillanders DT, Simpson SG, Taylor MA. A systematic review of the evidence base for schema therapy. Cognitive Behaviour Therapy. 2012; 41(3):185-202. [DOI:10.1080/16506073.2011.614274] [PMID]
Hinrichsen H, Waller G, Emanuelli F. Social anxiety and agoraphobia in the eating disorders: associations with core beliefs. The Journal of Nervous and Mental Disease. 2004; 192(11):784-7. [DOI:10.1016/j.eatbeh.2004.04.008] [PMID]
Boone L, Braet C, Vandereycken W. Are maladaptive schema domains and perfectionism related to body image concerns in eating disorder patients. European Eating Disorders Review. 2013: 21(1):45-51. [DOI:10.1002/erv.2175] [PMID]
Shafran R, Mansel W. Perfectionism psychopathology: A review of research and treatment. Clinical Psychology Review. 2001; 21:819-906. [DOI:10.1016/S0272-7358(00)00072-6]
Choo SY, Cha CKY. Predicting eating problems among Malaysian Chinese: Differential roles of positive and negative perfectionism. Personality and individual differences. 2013; 54(6):744-9. [DOI:10.1016/j.paid.2012.11.036]
Rabiei M, Mulkens S, Kalantari M, Molavi H, Bahrami F. Metacognitive therapy for body dysmorphic disorder patients in Iran: acceptability and proof of concept. Journal of behavior therapy and experimental psychiatry. 2012; 43(2):724-9. [DOI:10.1016/j.jbtep.2011.09.013] [PMID]
Veale D, Anson M, Miles S, Pieta M, Costa A, Ellison N. Efficacy of cognitive behaviour therapy versus anxiety management for body dysmorphic disorder: a randomised controlled trial. Psychotherapy and psychosomatics. 2014; 83(6):341-53. [DOI:10.1159/000360740] [PMID]
Zeinodini Z, Sedighi S, Rahimi MB, Noorbakhsh S, Esfahani SR. Dysfunctional metacognitive beliefs in body dysmorphic disorder. Global journal of health science. 2016; 8(3):10. [DOI:10.5539/gjhs.v8n3p10] [PMID] [PMCID]
Harrison A, de la Cruz LF, Enander J, Radua J, Mataix-Cols D. Cognitive-behavioral therapy for body dysmorphic disorder: A systematic review and meta-analysis of randomized controlled trials. Clinical Psychology Review. 2016; 48:43-51. [DOI:10.1016/j.cpr.2016.05.007] [PMID]
Fisak B, Mentuccia M, Przeworski A. Meta-worry in adolescents: Examination of the psychometric properties of the meta-worry questionnaire in an adolescent sample. Behavioural and cognitive psychotherapy. 2014; 42(4):491-6. [DOI:10.1017/S1352465813000374] [PMID]
Benedict C, Rodriguez VM, Carter J, Temple L, Nelson C, Duhamel K. Investigation of body image as a mediator of the effects of bowel and GI symptoms on psychological distress in female survivors of rectal and anal cancer. Support Care Cancer. 2016; 24(4):1795-802. [DOI:10.1007/s00520-015-2976-2] [PMID] [PMCID]
Hofmann SG, Asnaani A, Vonk IJ, Sawyer AT, Fang A. The efficacy of cognitive behavioral therapy: A review of meta-analyses. Cognitive therapy and research. 2012; 36(5):427-40. [DOI:10.1007/s10608-012-9476-1] [PMID] [PMCID]
Martens U, Czerwenka S, Schrauth M, Kowalski A, Enck P, Hartmann M, et al. Body image and psychiatric comorbidity in patients with somatoform gastrointestinal disorders. Zeitschrift fur Psychosomatische Medizin und Psychotherapie. 2010; 56(1):47-55. [DOI:10.13109/zptm.2010.56.1.47] [PMID]
Kriston L, Schäfer J, Jacob GA, Härter M, Hölzel LP. Reliability and validity of the German version of the Young Schema Questionnaire-Short Form 3 (YSQ-S3). European Journal of Psychological Assessment. 2013; 29:205-12. [DOI:10.1027/1015-5759/a000143]
Welburn K, Coristine M, Dagg P, Pontefract A, Jordan SH. The schema questionnaire - short form: factor analysis and the relationship between schemas and symptoms. Cognitive Therapy and Research. 2002: 26(4):519-30. [DOI:10.1023/A:1016231902020]
Williams J, Hadjistavropoulos T, Sharpe D. A meta-analysis of psychological and pharmacological treatments for body dysmorphic disorder. Behaviour Research and Therapy. 2006; 44(1):99-111. [DOI:10.1016/j.brat.2004.12.006] [PMID]
Shafrana R, Rachman S. Thought-action fusion: a review. Journal of Behavior Therapy and Experimental Psychiatry. 2004; 35(4):87-107. [DOI:10.1016/j.jbtep.2004.04.002] [PMID]
Kung CS, Chan CK. Differential roles of positive and negative perfectionism in predicting occupational eustress and distress. Personality and Individual differences. 2014; 58:76-81. [DOI:10.1016/j.paid.2013.10.011]
Short MM, Mazmanian D. Perfectionism and negative repetitive thoughts: Examining a multiple mediator model in relation to mindfulness. Personality and Individual Differences. 2013; 55(6):716-21. [DOI:10.1016/j.paid.2013.05.026]
Spielberger CD, Gonzalez-Reigosa F, Martinez-Urrutia A, Natalicio LF, Natalicio DS. The state-trait anxiety inventory. Revista Interamericana de Psicologia/Interamerican. Journal of Psychology. 2010; 17(5):3-4. [DOI:10.1002/9780470479216.corpsy0943]
Sadati L, Pazouki A, Mehdizadeh A, Shoar S, Tamannaie Z, Chaichian S. Effect of preoperative nursing visit on preoperative anxiety and postoperative complications in candidates for laparoscopic cholecystectomy: A randomized clinical trial. Scandinavian journal of caring sciences. 2013; 27(4):994-8. [DOI:10.1111/scs.12022] [PMID]
Whiting SE, May AC, Rudy BM, Davis TE. Strategies for the control of unwanted thoughts in adolescents: The Adolescent Thought Control Questionnaire (TCQ-A). Journal of Psychopathology and Behavioral Assessment. 2014; 36(2):276-87. [DOI:10.1007/s10862-013-9369-y]
Gillanders DT, Bolderston H, Bond FW, Dempster M, Flaxman PE, Campbell L, et al. The development and initial validation of the cognitive fusion questionnaire. Behavior therapy. 2014; 45(1):83-101. [DOI:10.1016/j.beth.2013.09.001] [PMID]
Bridges KR. Using attributional style to predict academic performance: How does it compare to traditional methods. Personality and individual differences. 2001; 31:723-30. [DOI:10.1016/S0191-8869(00)00174-4]
Fingeret MC, Teo I, Epner DE. Managing body image difficulties of adult cancer patients: lessons from available research. Cancer. 2014; 120(5):633-41. [DOI:10.1002/cncr.28469] [PMID] [PMCID]
Normann N, van Emmerik AA, Morina N. The efficacy of metacognitive therapy for anxiety and depression: A meta‐analytic review. Depression and Anxiety. 2014; 31(5):402-11. [DOI:10.1002/da.22273] [PMID]
Elliott R, Zahn R, Deakin JW, Anderson IM. Affective cognition and its disruption in mood disorders. Neuropsychopharmacology. 2011; 36(1):153. [DOI:10.1038/npp.2010.77] [PMID] [PMCID]
Collins B, Gonzalez D, Gaudilliere DK, Shrestha P, Girod S. Body dysmorphic disorder and psychological distress in orthognathic surgery patients. Journal of Oral and Maxillofacial Surgery. 2014; 72(8): 1553-8. [DOI:10.1016/j.joms.2014.01.011] [PMID]
Dykas MJ, Cassidy J. Attachment and the processing of social information across the life span: Theory and evidence. Psychological bulletin. 2011; 137(1):19. [DOI:10.1037/a0021367] [PMID]
Dimaggio G, Popolo R, Salvatore G. Formulation of functioning for avoidant personality disorder in metacognitive interpersonal therapy. In: Kramer U, editor. Case Formulation for Personality Disorders. Massachusetts: Academic Press; 2019. [DOI:10.1016/B978-0-12-813521-1.00008-4]
Cormier A, Jourda B, Laros C, Walburg V, Callahan S. Influence between early maladaptive schemas and depression. L’Encéphale, 2010; 37(4):293-8. [DOI:10.1016/j.encep.2011.01.001] [PMID]
Wells A, Carter K. Further tests of a cognitive model of generalized anxiety disorder: Meta-cognitions and worry in GAD, panic disorder, social phobia, depression, and nonpatients. Behavior Therapy. 2001; 32:85-102. [DOI:10.1016/S0005-7894(01)80045-9]
Lambert KG. Rising rates of depression in today’s society: Consideration of the roles of effort-based rewards and enhanced resilience in day-to-day functioning. Neuroscience & Biobehavioral Reviews. 2006; 30(4):497-510. [DOI:10.1016/j.neubiorev.2005.09.002] [PMID]
Grøtte T, Solem S, Vogel PA, Güzey IC, Hansen B, Myers SG. Metacognition, responsibility, and perfectionism in obsessive-compulsive disorder. Cognitive Therapy and Research. 2015; 39(1):41-50. [DOI:10.1007/s10608-014-9635-7]
Moulding R, Kyrios M. Anxiety disorders and control related beliefs: The exemplar of Obsessive-Compulsive Disorder (OCD). Clinical Psychology Review. 2006; 26(5):573-83. [DOI:10.1016/j.cpr.2006.01.009] [PMID]
Saboonchi F, Lundh LG. Perfectionism, anger, somatic health, and positive effect. Personality and Individual Differences. 2003; 35:1585-99. [DOI:10.1016/S0191-8869(02)00382-3]
Limburg K, Martin S, Hagger S, Egan J. The relationship between perfectionism and psychopathology: A meta‐analysis. Journal of Clinical Psychology. 2017; 73(10):1301-26. [DOI:10.1002/jclp.22435] [PMID]
Article Type: Research Article |
Subject:
Cognition
Received: 2018/06/24 | Accepted: 2018/09/2 | Published: 2018/11/1
Received: 2018/06/24 | Accepted: 2018/09/2 | Published: 2018/11/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Hamadan University of Medical Sciences.
Published by UMSHA Press
Journal Tel: +989025126654
Publisher Tel: +985138419434
Website: http://ajnpp.umsha.ac.ir
Email: avicennajnpp[at]gmail.com
